Report: Reproductive
Technology
The President’s Council on
Bioethics
Chapter
1. Biotechnology and the Pursuit of Happiness: An Introduction
Chapter
3. Superior Performance
Chapter
6. “Beyond Therapy”: General Reflections
==============================
Reproduction and
Responsibility: The Regulation of New Biotechnologies
The President’s Council on Bioethics
Washington, D.C., March 2004
==============================
Letter of Transmittal
The President’s Council on Bioethics
1801 Pennsylvania Avenue, N.W., Suite 700
Washington, D.C. 20006
March 31, 2004
The President
The White House
Washington, D.C.
Dear Mr. President:
I am pleased to present to you Reproduction and
Responsibility: The Regulation of New Biotechnologies, the latest report of
the President’s Council on Bioethics, and one that contains a set of unanimous
policy recommendations. The product of two years of research, reflection, and
deliberation, we hope that it will prove a worthy contribution to understanding
and addressing important ethical and social issues arising at the intersection
of assisted reproduction and genetic knowledge.
This report differs from, yet complements, the Council’s
work in its previous publications. In Human Cloning and Human Dignity,
we addressed the limited topic of human cloning—what to think and what to do
about it—and offered specific legislative recommendations. In Monitoring
Stem Cell Research, we answered your request for an update on developments
concerning human stem cell research, both in basic and clinical research and in
the ethical and policy debates, as these have emerged under the current federal
policy. In Beyond Therapy: Biotechnology and the Pursuit of Happiness,
we surveyed growing capacities that biotechnologies are providing to serve
non-medical goals—such as the desires for “better children,” “superior
performance,” “ageless bodies,” and “happy souls”—and sought to raise public
awareness of the challenges such pursuits might pose to the meaning of our
humanity. And in Being Human, we offered a rich anthology of readings to
help the nation better appreciate and promote those aspects of our humanity
affected by the coming age of biotechnology. Only in this report do we address
the large social and political question: how can we monitor, oversee, and
regulate these burgeoning new technologies, so as to reap their benefits while
avoiding their harms, both overt and subtle? How can we exercise responsible
control over where biotechnology may be taking us, in order to both serve and
preserve our humanity?
In investigating the general subject of the regulation of
biotechnology, we have taken as our specific focus the intersection of the
technologies of assisted reproduction, human genomic knowledge and technique,
and human embryo research. Advances in biotechnology are providing new
capacities for altering and influencing the beginnings of human life,
especially life initiated outside the body, in the clinic, or in the
laboratory. The well-established procedures of in vitro fertilization are being
rapidly augmented by abilities to test the genetic make-up of embryos, to
screen them for genetic diseases, to select them for their sex or (in the
future) for some other desired traits, and to alter them in many other ways.
These new capacities increase the variety and complexity of the options facing
infertile couples and others seeking assisted reproduction, and they raise the
prospect of changes in human reproduction that may have great significance not
only for the parents and children involved, but also for society as a whole.
The Council has sought to understand the public policy
implications of these developments in human reproduction and, in particular,
the ways in which the technologies in question are currently monitored and
regulated. Surveying this domain in our report on human cloning, we noted that
we lack comprehensive knowledge about what is being done, with what success, at
what risk, under what ethical guidelines, respecting which moral boundaries,
subject to what oversight and regulation, and with what sanctions for
misconduct or abuse. If we are to have wise public policy regarding these
scientifically and medically promising but morally challenging activities, we
need careful study and sustained public moral discourse on this general
subject, and not only on specific narrowly defined pieces of the field.
Since the release of that report, the Council has conducted
a comprehensive inquiry into the current regulation of those biotechnologies
that touch on human reproduction. This report is the fruit of that inquiry.
The Council finds that our regulatory institutions have not
kept pace with our rapid technological advance. Indeed, there is today no
public authority responsible for monitoring or overseeing how these
technologies make their way from the experimental to the clinical stage, from
novel approach to widespread practice. There is no authority, public or
private, that monitors how or to what extent these new technologies are being
or will be used, or that is responsible for attending to the ways they affect
the health and well-being of the participants or the character of human
reproduction more generally. Our existing regulatory institutions, such as the
Food and Drug Administration or local institutional review boards, do not at
the present time oversee this area, and the welcome ethical standards
promulgated by the professional societies are somewhat limited in scope and not
binding on individual member practitioners.
Yet the Council has refrained, at least for the time being,
from proposing major new regulatory institutions. Gaps in our current
information make doing so premature, and our deep differences over the moral
status of human embryos make it problematic. Before either policymakers or the
public can address the need for institutional change, we first need much more
additional information. What are the true health effects of assisted
reproductive technologies on children, mothers, and egg-donors? Are assisted-reproduction
patients able to make fully informed choices in the current environment? Could
federal intervention be rendered unnecessary by better professional
self-regulation? What would be the benefits and the costs of each of the
various alternatives either for expanding the responsibilities of our current
regulatory institutions or for designing new ones, so as to provide oversight
and guidance for responsible practices in reproductive medicine and research?
The Council presents a series of recommendations—addressed both to government
and to the relevant scientific and medical practitioners—for data gathering,
reporting, and professional self-scrutiny. These recommendations are designed
to help us get answers to those and other such questions.
But even as we seek answers to these questions and ponder
the need for institutional reforms, we do think that the nation would benefit
from a series of targeted interim legislative measures that would safeguard
certain important ethical boundaries. Accordingly, we propose a series of
modest yet precise legislative proposals targeting certain unethical or
disquieting practices in human reproduction—for example, attempts to conceive
children other than by the union of egg and sperm, to produce a hybrid
animal-human embryo, to initiate a human pregnancy for any purpose other than
to produce a live-born child, or to try to grow human embryos in the bodies of
animals. (The full list of the targeted legislative measures—and of all the
other recommendations—is provided in the Executive Summary.) Based on our
deliberations to date, we believe these targeted measures will find support on
all sides—pro-choice as well as pro-life, secular as well as religious,
scientist as well as humanist, left as well as right. Like the nation at large,
our members hold differing views about certain foundational questions,
especially the moral standing of human embryos. Yet despite our great
differences, we all support these proposals and urge their swift adoption.
The issues surrounding the beginnings of human life are
notoriously controversial in our country, as they are on the Council. By
design, this Council consists of Members with strongly held yet divergent views
on these subjects. Yet precisely because of these differences, we have sought
in this report—and especially in its recommendations—to find a common ground in
certain aims and formulations that all sides could accept, without anyone
having to compromise on a matter of principle or having to repudiate what they
have said in previous reports. Rather than allow continuing disagreements to
blind us to possible significant points of agreement, we have sought precisely
to find those goods we all hold dear and to highlight them for the country, so
that some progress might be made where it is possible, while public debate and
attempts at persuasion continue on the issues that still divide us.
The Council stands behind these recommendations
unanimously, even though different members come to them from different premises
and with different aims and hopes—as they articulate in their personal
statements in the appendix to this document. This discernment of practical
common ground in the midst of meaningful disagreement and debate is an
accomplishment of which the Council is very proud. We hope it might point the
way for others to seek and find the responsible way forward in this vexing
arena of public policy.
As with our past reports, so in this one we have sought to
be—and we hope you will find us—fair in our approach, precise in our language,
accurate in our presentation, and thoughtful in our recommendations.
And as always, Mr. President, I send you this report with
the good wishes of my Council colleagues and our fine staff. Once again, we
thank you for the opportunity to serve.
Sincerely,
Leon R. Kass, M.D.
Chairman
==============================
Members of the Council
Leon R. Kass, M.D., Ph.D., Addie Clark Harding Professor, The College and the Committee on Social Thought, University of Chicago. Hertog Fellow, American Enterprise Institute.
Benjamin S. Carson, Sr., M.D.* Professor and Director of Pediatric Neurosurgery, Johns Hopkins Medical Institutions.
Rebecca S. Dresser, J.D., M.S. Daniel Noyes Kirby Professor of Law and Professor of Ethics in Medicine, Washington University, St. Louis.
Daniel W. Foster, M.D. John Denis McGarry, Ph.D. Distinguished Chair in Diabetes and Metabolic Reasearch, University of Texas Southwestern Medical School.
Francis Fukuyama, Ph.D. Dean of the Faculty, Bernard Schwartz Professor of International Political Economy, Paul H. Nitze School of Advanced International Studies, Johns Hopkins University.
Michael S. Gazzaniga, Ph.D. Dean of the Faculty, David T. McLaughlin Distinguished Professor, Professor of Psychological and Brain Sciences, Dartmouth College.
Robert P. George, J.D., D.Phil. McCormick Professor of Jurisprudence, Director of the James Madison Program in American Ideals and Institutions, Princeton University.
Mary Ann Glendon, J.D., M. Comp. L. Learned Hand Professor of Law, Harvard University.
Alfonso Gómez-Lobo, Dr. phil. Ryan Family Professor of Metaphysics and Moral Philosophy, Georgetown University.
William B. Hurlbut, M.D. Consulting Professor in Human Biology, Stanford University.
Charles Krauthammer, M.D. Syndicated Columnist.
Peter A. Lawler, Ph.D.* Chairman of the Department of Government and International Studies, Dana Professor of Government, Berry College.
Paul McHugh, M.D. University Distinguished Service Professor of Psychiatry, Johns Hopkins School of Medicine. Professor, Department of Mental Health, Bloomberg School of Public Health, Johns Hopkins University.
Gilbert C. Meilaender, Ph.D. Phyllis & Richard Duesenberg Professor of Christian Ethics, Valparaiso University.
Janet D. Rowley, M.D. Blum-Riese Distinguished Service Professor of Medicine, Molecular Genetics and Cell Biology, and Human Genetics, Pritzker School of Medicine, University of Chicago.
Michael J. Sandel, D.Phil. Anne T. and Robert M. Bass Professor of Government, Harvard University.
Diana J. Schaub, Ph.D.* Chairman of the Department of Political Science, Loyola College, Maryland.
James Q. Wilson, Ph.D.
James A. Collins Professor of Management and Public Policy Emeritus, University of California-Los Angeles. Reagan Professor of Public Policy, Pepperdine University.
==============================
Council Staff and Consultants
Dean Clancy
Executive Director
Allison Arensman
Intern
Peter Berkowitz
Senior Consultant
Karen Blackistone
Staff Assistant
Eric Cohen
Senior Research Consultant
Judith Crawford
Administrative Director
Dov Fox
Intern
Diane M. Gianelli
Director of Communications
Katie Goodman
Intern
Laura Harmon, Esq.
Projects Administrator
Emily Jones
Executive Administrator
Joshua Kleinfeld
Senior Research Analyst
Yuval Levin
Senior Research Analyst
Nelson Moussazadeh
Intern
Michelle Powers
Law Clerk
Richard Roblin, Ph.D.
Scientific Director
Adam Schulman
Research Consultant
O. Carter Snead, Esq.
General Counsel
Catherine Thorp
Staff Assistant/Receptionist
Audrea R. Vann
Information Tech. Assistant
Rachel Flick Wildavsky
Director, Education Project
Adam Wolfson
Consultant
Lee L. Zwanziger, Ph.D.
Director of Research
==============================
Preface
Beyond Therapy: Biotechnology and the Pursuit of Happiness
is a report of the President’s Council on Bioethics, which was created by
President George W. Bush on November 28, 2001, by means of Executive Order
13237.
The Council’s purpose is to advise the President on
bioethical issues related to advances in biomedical science and technology. In
connection with its advisory role, the mission of the Council includes the
following functions:
- To undertake fundamental inquiry into the human and moral significance of developments in biomedical and behavioral science and technology.
- To explore specific ethical and policy questions related to these developments.
- To provide a forum for a national discussion of bioethical issues.
- To facilitate a greater understanding of bioethical issues.
President Bush left the Council free to establish its own
priorities among the many issues encompassed within its charter, and to
determine its own modes of proceeding.
In keeping with our mission, we have undertaken an inquiry
into the potential implications of using biotechnology “beyond therapy,” in
order to try to satisfy deep and familiar human desires: for better children,
superior performance, ageless bodies, and happy souls. Such uses of
biotechnology, some of which are now possible and some of which may become
possible in the future, are likely to present us with profound and highly
consequential ethical challenges and choices. They may play a crucial role in
shaping human experience in the fast-approaching age of biotechnology.
We believe that the promises and perils of this prospect
merit the attention of the nation. They are a worthy target for fundamental
inquiry, an appropriate arena for exploring specific ethical questions, an
important subject for ongoing national discussion, and (through such
discussion) perhaps also a means of facilitating greater understanding of
bioethical issues. Our intention in this report is to clarify the relevant
scientific possibilities and, especially, to explore the ethical and social
implications of using biotechnical powers for purposes beyond therapy.
The Council has been attentive to this subject from its
very earliest days, beginning with a discussion at its first meeting, in
January of 2002, of the purposes and motivations underlying biomedical science.
The Council has also devoted time expressly to this particular project at nine
of its meetings in the past two years (in April, July, September, October, and
December of 2002, and in January, March, June, and July of 2003), taking
testimony from experts in the relevant scientific, ethical, and social arenas,
receiving public comment, and engaging in serious deliberation among the
Members. All told, twenty-two sessions, of ninety minutes each, were devoted to
the subject at public meetings. Complete transcripts of all these sessions are
available to the public on the Council’s website at www.bioethics.gov.
This report draws directly upon those sessions and
discussions, as well as on written material prepared by some Council members
and staff during the process. Given that context, it is crucial to understand
the precise nature of this document: The final document is not a research
report, but an ethical inquiry. It makes no pretense of comprehensiveness; it
does not report exhaustively on the literature, scientific or ethical. Rather,
it aspires to thoughtful reflection and represents mainly a (partial)
distillation of the Council’s own thinking. Not every Member shares every
concern here expressed, or every scientific speculation or ethical assessment
offered, and a few disagreements on particular points are noted in the text.
Different Members care more about different topics, and all of us are aware
that there are issues not addressed, and scientific opinions and ethical
viewpoints not reflected. Yet, as a Council, we offer the entire document as a
guide to further thinking on this very important subject.
We hope, through this report, to advance the nation’s
awareness and understanding of a critical set of bioethical issues and to bring
them beyond the narrow circle of bioethics professionals into the larger public
arena, where questions of such consequence rightly belong.
In creating this Council, President Bush expressed his
desire to see us
consider all of the medical and ethical ramifications of
biomedical innovation. . . . This council will keep us apprised of new
developments and give our nation a forum to continue to discuss and evaluate
these important issues. As we go forward, I hope we will always be guided by
both intellect and heart, by both our capabilities and our conscience.
It has been our goal in the present report, as in all of
our work, to live up to these high hopes and noble aspirations.
LEON R. KASS, M.D.
Chairman
==============================
Chapter
1. Biotechnology and the Pursuit of Happiness: An
Introduction
Before reaching
these questions, we had better specify what we mean by “biotechnology,” for it
is a new word for our new age. Though others have given it both narrow and
broad definitions,i
our purpose—for reasons that will become clear—recommends that we work with a
very broad meaning: the processes and products (usually of industrial scale)
offering the potential to alter and, to a degree, to control the phenomena of
life—in plants, in (non-human) animals, and, increasingly, in human beings (the
last, our exclusive focus here). Overarching the processes and products it
brings forth, biotechnology is also a conceptual and ethical outlook,
informed by progressive aspirations. In this sense, it appears as a most recent
and vibrant expression of the technological spirit, a desire and disposition
rationally to understand, order, predict, and (ultimately) control the events
and workings of nature, all pursued for the sake of human benefit.
Thus understood, biotechnology is bigger than its processes
and products; it is a form of human empowerment. By means of its techniques
(for example, recombining genes), instruments (for example, DNA sequencers),
and products (for example, new drugs or vaccines), biotechnology empowers us human
beings to assume greater control over our lives, diminishing our subjection to
disease and misfortune, chance and necessity. The techniques, instruments, and
products of biotechnology—like similar technological fruit produced in other
technological areas—augment our capacities to act or perform effectively, for
many different purposes. Just as the automobile is an instrument that confers
enhanced powers of “auto-mobility” (of moving oneself), which powers can
then be used for innumerable purposes not defined by the machine itself, so DNA
sequencing is a technique that confers powers for genetic screening that can be
used for various purposes not determined by the technique; and synthetic growth
hormone is a product that confers powers to try to increase height in the short
or to augment muscle strength in the old. If we are to understand what
biotechnology is for, we shall need to keep our eye more on the new abilities
it provides than on the technical instruments and products that make the
abilities available to us.ii
This terminological discussion exposes the first
complication regarding the purposes of biotechnology: the fact that means and
ends are readily detached from one another. As with all techniques and the
powers they place in human hands, the techniques and powers of biotechnology
enjoy considerable independence from ties to narrow or specific goals.
Biotechnology, like any other technology, is not for anything in particular.
Like any other technology, the goals it serves are supplied neither by the
techniques themselves nor by the powers they make available, but by their human
users. Like any other means, a given biotechnology once developed to serve one
purpose is frequently available to serve multiple purposes, including some that
were not imagined or even imaginable by those who brought the means into being.
Second, there are several questions regarding the overall
goal of biotechnology: improving the lot of humankind. What exactly is it about
the lot of humankind that needs or invites improvement? Should we think only of
specific, as-yet-untreatable diseases that compromise our well-being, such
ailments as juvenile diabetes, cancer, or Alzheimer disease? Should we not also
include mental illnesses and infirmities, from retardation to major depression,
from memory loss to melancholy, from sexual incontinence to self-contempt? And
should we consider in addition those more deep-rooted limitations built into our
nature, whether of body or mind, including the harsh facts of decline, decay,
and death? What exactly is it about “man’s estate” that most calls for relief?
Just sickness and suffering, or also such things as nastiness, folly, and
despair? Must “improvement” be limited to eliminating these and other evils, or
should it also encompass augmenting our share of positive goods—beauty,
strength, memory, intelligence, longevity, or happiness itself?
Third, even assuming that we could agree on which aspects of
the human condition call for improvement, we would still face difficulties
deciding how to judge whether our attempts at improving them really made things
better—both for the individuals and for the society. Some of the goals we seek
might conflict with each other: longer life might come at the price of less
energy; superior performance for some might diminish self-esteem for others.
Efforts to moderate human aggression might wind up sapping ambition;
interventions aimed at quieting discontent might flatten aspiration. And,
unintended consequences aside, it is not easy to say just how much less
aggression or discontent would be good for us. Once we go beyond the treatment
of disease and the pursuit of health, there seem to be no ready-made or
reliable standards of better and worse available to guide our choices.
As this report will demonstrate, these are not idle or
merely academic concerns. Indeed, some are already upon us. We now have
techniques to test early human embryos for the presence or absence of many
genes: shall we use these techniques only to prevent disease or also to try to
get us “better” children? We are acquiring techniques for boosting muscle
strength and performance: shall we use them only to treat muscular dystrophy
and the weak muscles of the elderly or also to enable athletes to attain
superior performance? We are gradually learning how to control the biological
processes of aging: should we seek only to diminish the bodily and mental
infirmities of old age or also to engineer large increases in the maximum human
lifespan? We are gaining new techniques for altering mental life, including
memory and mood: should we use them only to prevent or treat mental illness or
also to blunt painful memories of shameful behavior, transform a melancholic
temperament, or ease the sorrows of mourning? Increasingly, these are exactly
the kinds of questions that we shall be forced to face as a consequence of new
biotechnical powers now and soon to be at our disposal. Increasingly we must
ask, “What is biotechnology for?” “What should it be for?”
I. The Golden
Age: Enthusiasm and Concern
By all accounts, we have entered upon a golden age for
biology, medicine, and biotechnology. With the completion of (the DNA
sequencing phase of) the Human Genome Project and the emergence of stem cell
research, we can look forward to major insights into human development, normal
and abnormal, as well as novel and more precisely selected treatments for human
diseases. Advances in neuroscience hold out the promise of powerful new
understandings of mental processes and behavior, as well as remedies for
devastating mental illnesses. Ingenious nanotechnological devices, implantable
into the human body and brain, raise hopes for overcoming blindness and
deafness, and, more generally, of enhancing native human capacities of
awareness and action. Research on the biology of aging and senescence suggests
the possibility of slowing down age-related declines in bodies and minds, and
perhaps even expanding the maximum human lifespan. In myriad ways, the
discoveries of biologists and the inventions of biotechnologists are steadily
increasing our power ever more precisely to intervene into the workings of our
bodies and minds and to alter them by rational design.
For the most part, there is great excitement over and
enthusiasm for these developments. Even before coming to the practical
benefits, we look forward to greatly enriched knowledge of how our minds and
bodies work. But it is the promised medical benefits that especially excite our
admiration. Vast numbers of people and their families ardently await cures for
many devastating diseases and eagerly anticipate relief from much human misery.
We will surely welcome, as we have in the past, new technological measures that
can bring us healthier bodies, decreased pain and suffering, peace of mind, and
longer life.
At the same time, however, the advent of new biotechnical
powers is for many people a cause for concern. First, the scientific findings
themselves raise challenges to human self-understanding: people wonder, for
example, what new knowledge of brain function and behavior will do to our
notions of free will and personal moral responsibility, formed before the
advent of such knowledge. Second, the prospect of genetic engineering, though
welcomed for treatment of inherited genetic diseases, raises for some people
fears of eugenics or worries about “designer babies.” Psychotropic drugs,
though welcomed for treatment of depression or schizophrenia, raise fears of
behavior control and worries about diminished autonomy or confused personal
identity. Precisely because the new knowledge and the new powers impinge
directly upon the human person, and in ways that may affect our very humanity,
a certain vague disquiet hovers over the entire enterprise. Notwithstanding the
fact that almost everyone, on balance, is on the side of further progress, the
new age of biotechnology will bring with it novel, and very likely momentous,
challenges.
While its leading benefits and blessings are readily identified,
the ethical and social concerns raised by the march of biotechnology are not
easily articulated. They go beyond the familiar issues of bioethics, such as
informed consent for human subjects of research, equitable access to the fruits
of medical research, or, as with embryo research, the morality of the means
used to pursue worthy ends. Indeed, they seem to be more directly connected to
the ends themselves, to the uses to which biotechnological powers will be put.
Generally speaking, these broader concerns attach especially to those uses of
biotechnology that go “beyond therapy,” beyond the usual domain of medicine and
the goals of healing, uses that range from the advantageous to the frivolous to
the pernicious. Biotechnologies are already available as instruments of
bioterrorism (for example, genetically engineered super-pathogens or drugs that
can destroy the immune system or erase memory), as agents of social control
(for example, tranquilizers for the unruly or fertility-blockers for the impoverished),
and as means to improve or perfect our bodies and minds and those of our
children (steroids for body-building or stimulants for taking exams). In the
first two cases, there are concerns about what others might do to us, or what
some people, including governments, might do to other people. In the last case,
there are concerns about what we might voluntarily do to ourselves or to our
society. People worry both that our society might be harmed and that we
ourselves might be diminished in ways that could undermine the highest and
richest possibilities for human life.
Truth to tell, not everyone who has considered these
prospects is worried. On the contrary, some celebrate the perfection-seeking
direction in which biotechnology may be taking us. Indeed, some scientists and
biotechnologists have not been shy about prophesying a
better-than-currently-human world to come, available with the aid of genetic
engineering, nanotechnologies, and psychotropic drugs. “At this unique moment
in the history of technical achievement,” declares a recent report of the
National Science Foundation, “improvement of human performance becomes
possible,” and such improvement, if pursued with vigor, “could achieve a golden
age that would be a turning point for human productivity and quality of life.”1“Future
humans—whoever or whatever they may be—will look back on our era as a
challenging, difficult, traumatic moment,” writes a scientist observing present
trends. “They will likely see it as a strange and primitive time when people
lived only seventy or eighty years, died of awful diseases, and conceived their
children outside a laboratory by a random, unpredictable meeting of sperm and
egg.”2
James Watson, co-discoverer of the structure of DNA, put the matter as a simple
question: “If we could make better human beings by knowing how to add genes,
why shouldn’t we?”3
Yet the very insouciance of some of these predictions and
the confidence that the changes they endorse will make for a better world
actually serve to increase public unease. Not everyone cheers a summons to a “post-human”
future. Not everyone likes the idea of “remaking Eden” or of “man playing God.”
Not everyone agrees that this prophesied new world will be better than our own.
Some suspect it could rather resemble the humanly diminished world portrayed in
Aldous Huxley’s novel Brave New World, whose technologically enhanced
inhabitants live cheerfully, without disappointment or regret, “enjoying” flat,
empty lives devoid of love and longing, filled with only trivial pursuits and
shallow attachments.
II. The Case
for Public Attention
Despite the disquiet it arouses, the subject of using
biomedical technologies for purposes “beyond therapy” has received remarkably
little public attention. Given its potential importance, it is arguably the
most neglected topic in public bioethics. No previous national bioethics
commission has considered the subject, and for understandable reasons. The
realm of biotechnology “beyond therapy” is hard to define, a gray zone where judgment
is, to say the least, difficult. Compared with more immediate topics in
bioethics, the questions raised by efforts to “improve on human nature” seem
abstract, remote, and overly philosophical, unfit for public policy; indeed,
many bioethicists and intellectuals believe either that there is no such thing
as “human nature” or that altering it is not ethically problematic. The
concerns raised are complicated and inchoate, hard to formulate in general
terms, especially because the differing technologically based powers raise
different ethical and social questions: enhancing athletic performance with
steroids and genetic selection of embryos for reproduction give rise to
different concerns. Analysis often requires distinguishing the primary and
immediate uses of a technology (say, mood-elevating drugs to treat depression
or memory-blunting drugs to prevent post-traumatic stress disorder) from
derivative and longer-term uses and implications (the same drugs used as
general mood-brighteners or to sanitize memories of shameful or guilty
conduct). Speculation about those possible implications, never to be confused
with accurate prediction, is further complicated by the fact that the meaning
of any future uses of biotechnology “beyond therapy” will be determined at
least as much by the goals and practices of an ever-changing society as by the
technologies themselves. Finally, taking up these semi-futuristic prospects may
seem a waste of public attention, especially given the more immediate ethical
issues that clamor for attention. Some may take us to task for worrying about
the excesses and abuses of biotechnology and the dangers of a “brave new
world” when, in the present misery-ridden world, millions are dying of AIDS,
malaria, and malnutrition, in part owing to the lack of already
available biomedical technologies.
Yet despite these genuine difficulties and objections, we
believe that it is important to open up this subject for public discussion. For
it raises some of the weightiest questions in bioethics. It touches on the ends
and goals to be served by the acquisition of biotechnical power, not just on
the safety, efficacy, or morality of the means. It bears on the nature and
meaning of human freedom and human flourishing. It faces squarely the alleged
threat of dehumanization as well as the alleged promise of “super-humanization.”
It compels attention to what it means to be a human being and to be active
as a human being. And it is far from being simply futuristic: current
trends make clear how the push “beyond therapy” and “toward perfection and
happiness” is already upon us—witness the growing and increasingly acceptable
uses of cosmetic surgery, performance-enhancing drugs, and mood- or
attention-altering agents.iii
Given the burgeoning research in neuroscience and the ever-expanding biological
approaches to psychiatric disorders and to all mental states, it seems clear
that the expected new discoveries about the workings of the psyche and the
biological basis of behavior will surely increase both our ability and our
desire to alter and improve them. Decisions we are making today—for instance,
what to do about sex selection or genetic selection of embryos, or whether to prescribe
behavior-modifying drugs to preschoolers, or how vigorously to try to reverse
the processes of senescence—will set the path “beyond therapy” for coming
generations. And fair or not, the decisions and choices of the privileged or avant-garde
often will pave the way that others later follow, in the process sometimes
changing what counts as “normal,” often irreversibly.
Taking up this topic is, in fact, responsive to the charge
President Bush gave to this Council, formed by executive order “to advise the
President on bioethical issues that may emerge as a consequence of advances in
biomedical science and technology.” Among the specific functions set forth in
connection with our mission, the Council was instructed in the first place “to
undertake fundamental inquiry into the human and moral significance of
developments in biomedical and behavioral science and technology,” and then “to
explore specific ethical and policy questions related to these developments.”
Anticipating, as we do, the arrival of technological powers that are likely to
affect profoundly the nature, shape, and content of human experience, human
character, and human society, we believe that it is highly desirable that we
try to articulate as best we can their likely “human and moral significance.”
The Council has not only the mandate but also the
opportunity to take a more long-range view of these matters. Unlike legislators
caught up in the demands of pressing business, we have the luxury of being able
carefully and disinterestedly to consider matters before they become hotly
contested items for public policy. Unless a national bioethics council takes up
this topic, it is unlikely that anyone else in public life will do so. And if
we do not prepare ourselves in advance to think about these matters, we shall
be ill prepared to meet the challenges as they arrive and to make wisely the
policy decisions they may require.
III. Defining
the Topic
Having offered our reasons for taking up the topic, we need
next to define it more carefully and to indicate how we mean to approach it. As
already suggested, the “beyond therapy” uses of biotechnology on human beings
are manifold. We shall not here consider biotechnologies as instruments of
bioterrorism or of mass population control. The former topic is highly
specialized and tied up with matters of national security, an area beyond our
charge and competence. Also, although the practical and political difficulties
they raise are enormous, the ethical and social issues are relatively
uncomplicated. The main question about bioterrorism is not what to think about
it but how to prevent it. And the use of tranquilizing aerosols for crowd
control or contraceptive additions to the drinking water, unlikely prospects in
liberal democratic societies like our own, raise few issues beyond the familiar
one of freedom and coercion.
Much more ethically challenging are those “beyond therapy”
uses of biotechnology that would appeal to free and enterprising people, that
would require no coercion, and, most crucially, that would satisfy widespread
human desires. Sorting out and dealing with the ethical and social issues of
such practices will prove vastly more difficult since they will be intimately
connected with goals that go with, rather than against, the human grain. For
these reasons, we confine our attention to those well-meaning and strictly
voluntary uses of biomedical technology through which the user is seeking some
improvement or augmentation of his or her own capacities, or, from similar
benevolent motives, of those of his or her children. Such use of biotechnical
powers to pursue “improvements” or “perfections,” whether of body, mind,
performance, or sense of well-being, is at once both the most seductive and the
most disquieting temptation. It reflects humankind’s deep dissatisfaction with
natural limits and its ardent desire to overcome them. It also embodies what is
genuinely novel and worrisome in the biotechnical revolution, beyond the
so-called “life issues” of abortion and embryo destruction, important though
these are. What’s at issue is not the crude old power to kill the creature made
in God’s image but the attractive science-based power to remake ourselves after
images of our own devising. As a result, it gives unexpected practical urgency
to ancient philosophical questions: What is a good life? What is a good
community?
IV. Ends and
Means
Such a dream of human perfectibility by means of science
and technology has, in fact, been present from the start of modern science in
the seventeenth century. When René Descartes, in his famous Discourse on
Method, set forth the practical purpose for the new science he was
founding, he spoke explicitly of our becoming “like masters and owners of
nature” and outlined the specific goals such mastery of nature would serve:
This is desirable not only for the invention of an infinity
of artifices which would enable us to enjoy, without any pain, the fruits of
the earth and all the commodities to be found there, but also and principally
for the conservation of health, which is without doubt the primary good and the
foundation of all other goods in this life.
But, as the sequel makes clear, he has more than health in
mind:
For even the mind is so dependent on the temperament and on
the disposition of the organs of the body, that if it is possible to find some
means that generally renders men more wise and more capable than they
have been up to now, I believe that we must seek for it in medicine. . . .
[W]e could be spared an infinity of diseases, of the body as well as of the
mind, and even also perhaps the enfeeblement of old age, if we had
enough knowledge of their causes and all the remedies which nature has provided
us. (Emphasis added.)4
Descartes foresaw a new medicine, unlike any the world had
known, that would not only be able effectively to conserve health, but might
also improve human bodies and minds beyond what nature herself had granted us:
to make us wiser, more capable and competent, and perhaps even impervious to
aging and decay—in a word, to make us healthy and happy, indefinitely. Owing to
the powers now and soon to be available to us, Descartes’s dream no longer
seems a mere fantasy.
What exactly are the self-augmenting capabilities that we
are talking about? What kinds of technology make them possible? What sorts of
ends are they likely to serve? How soon will they be available? They are powers
that potentially affect the capacities and activities of the human body; the
capacities and activities of the mind or soul; and the shape of the human life
cycle, at both ends and in between. We already have powers to prevent fertility
and to promote it; to initiate life in the laboratory; to screen our genes,
both as adults and as embryos, and to select (or reject) nascent life based on
genetic criteria; to insert new genes into various parts of the adult body, and
perhaps someday also into gametes and embryos; to enhance muscle performance
and endurance; to alter memory, mood, appetite, libido, and attention through
psychoactive drugs; to replace body parts with natural organs, mechanical
organs, or tissues derived from stem cells, perhaps soon to wire ourselves
using computer chips implanted into the body and brain; and, in the foreseeable
future, to prolong not just the average but also the maximum human life
expectancy. The technologies for altering our native capacities are mainly
those of genetic screening and genetic engineering; drugs, especially
psychoactive ones; and the ability to replace body parts or to insert novel
ones. The availability of some of these capacities, using these techniques, has
been demonstrated only with animals; but others are already in use in humans.
It bears emphasis that these powers and technologies have
not been and are not being developed for the purpose of producing improved,
never mind perfect or post-human, beings. They have been produced largely for
the purposes of preventing and curing disease, reversing disabilities, and
alleviating suffering. Even the prospect of machine-brain interaction and
implanted nanotechnological devices starts with therapeutic efforts to enable
the blind to see and the deaf to hear. Yet the “dual use” aspect of most of
these powers—encouraged by the ineradicable human urge toward “improvement,”
exploited by the commercial interests that already see vast market
opportunities for nontherapeutic uses, and likely welcomed by many people
seeking a competitive edge in their strivings to “get ahead”—means that we must
not be lulled to sleep by the fact that the originators of these powers were no
friends to Brave New World. Once here, techniques and powers can produce
desires where none existed before, and things often go where no one ever
intended.
V. The
Limitations of the “Therapy vs. Enhancement” Distinction
Although, as we have indicated, the topic of the
biotechnological pursuit of human improvement has not yet made it onto the
agenda of public bioethics, it has received a certain amount of attention in
academic bioethical circles under the rubric of “enhancement,” understood in
contradistinction to “therapy.”5
Though we shall ourselves go beyond this distinction, it provides a useful
starting place from which to enter the discussion of activities that aim “beyond
therapy.”iv“Therapy,”
on this view as in common understanding, is the use of biotechnical power to
treat individuals with known diseases, disabilities, or impairments, in an
attempt to restore them to a normal state of health and fitness. “Enhancement,”
by contrast, is the directed use of biotechnical power to alter, by direct intervention,
not disease processes but the “normal” workings of the human body and psyche,
to augment or improve their native capacities and performances. Those who
introduced this distinction hoped by this means to distinguish between the
acceptable and the dubious or unacceptable uses of biomedical technology:
therapy is always ethically fine, enhancement is, at least prima facie,
ethically suspect. Gene therapy for cystic fibrosis or Prozac for major
depression is fine; insertion of genes to enhance intelligence or steroids for
Olympic athletes is, to say the least, questionable.
At first glance, the distinction between therapy and
enhancement makes good sense. Ordinary experience recognizes the difference
between “restoring to normal” and “going beyond the normal.” Also, as a
practical matter, this distinction seems a useful way to distinguish between
the central and obligatory task of medicine (healing the sick) and its marginal
and extracurricular practices (for example, Botox injections and other merely
cosmetic surgical procedures). Because medicine has, at least traditionally,
pursued therapy rather than enhancement, the distinction helps to delimit the
proper activities of physicians, understood as healers. And because physicians
have been given a more-or-less complete monopoly over the prescription and
administration of biotechnology to human beings, the distinction, by seeking to
circumscribe the proper goals of medicine, indirectly tries to circumscribe
also the legitimate uses of biomedical technology. Accordingly, it also helps
us decide about health care costs: health providers and insurance companies
have for now bought into the distinction, paying for treatment of disease, but
not for enhancements. More fundamentally, the idea of enhancement understood as
seeking something “better than well” points to the perfectionist, not to say
utopian, aspiration of those who would set out to improve upon human nature in
general or their own particular share of it.
But although the distinction between therapy and
enhancement is a fitting beginning and useful shorthand for calling attention
to the problem (and although we shall from time to time make use of it
ourselves), it is finally inadequate to the moral analysis. “Enhancement” is,
even as a term, highly problematic. In its most ordinary meaning, it is
abstract and imprecise.v
Moreover, “therapy” and “enhancement” are overlapping categories: all
successful therapies are enhancing, even if not all enhancements enhance by
being therapeutic. Even if we take “enhancement” to mean “nontherapeutic
enhancement,” the term is still ambiguous. When referring to a human function,
does enhancing mean making more of it, or making it better? Does it refer to
bringing something out more fully, or to altering it qualitatively? In what
meaning of the term are both improved memory and selective erasure of memory “enhancements”?
Beyond these largely verbal and conceptual ambiguities, there
are difficulties owing to the fact that both “enhancement” and “therapy” are
bound up with, and absolutely dependent on, the inherently complicated idea of
health and the always-controversial idea of normality. The differences between
healthy and sick, fit and unfit, are experientially evident to most people, at
least regarding themselves, and so are the differences between sickness and
other troubles. When we are bothered by cough and high fever, we suspect that
we are sick, and we think of consulting a physician, not a clergyman. By
contrast, we think neither of sickness nor of doctors when we are bothered by
money problems or worried about the threat of terrorist attacks. But there are
notorious difficulties in trying to define “healthy” and “impaired,” “normal”
and “abnormal” (and hence, “super-normal”), especially in the area of “behavioral”
or “psychic” functions and activities. Some psychiatric diagnoses—for example, “dysthymia,”
“oppositional disorder,” or “social anxiety disorder”—are rather vague: what is
the difference between extreme shyness and social anxiety? And, on the positive
side, mental health shades over into peace of mind, which shades over into
contentment, which shades over into happiness. If one follows the famous World
Health Organization definition of health as “a state of complete physical,
mental and social well-being,” almost any intervention aimed at enhancement may
be seen as health-promoting, and hence “therapeutic,” if it serves to promote
the enhanced individual’s mental well-being by making him happier.
Yet even for those using a narrower definition of health,
the distinction between therapy and enhancement will prove problematic. While
in some cases—for instance, a chronic disease or a serious injury—it is fairly
easy to point to a departure from the standard of health, other cases defy
simple classification. Most human capacities fall along a continuum, or a “normal
distribution” curve, and individuals who find themselves near the lower end of
the normal distribution may be considered disadvantaged and therefore unhealthy
in comparison with others. But the average may equally regard themselves as
disadvantaged with regard to the above average. If one is responding in both
cases to perceived disadvantage, on what principle can we call helping someone
at the lower end “therapy” and helping someone who is merely average “enhancement”?
In which cases of traits distributed “normally” (for example, height or IQ or
cheerfulness) does the average also function as a norm, or is the norm itself
appropriately subject to alteration?
Further complications arise when we consider causes of
conditions that clamor for modification. Is it therapy to give growth hormone
to a genetic dwarf, but not to a short fellow who is just unhappy to be short?
And if the short are brought up to the average, the average, now having become
short, will have precedent for a claim to growth hormone injections. Since more
and more scientists believe that all traits of personality have at least a
partial biological basis, how will we distinguish the biological “defect” that
yields “disease” from the biological condition that yields shyness or
melancholy or irascibility?
For these reasons, among others, relying on the distinction
between therapy and enhancement to do the work of moral judgment will not
succeed. In addition, protracted arguments about whether or not something is or
is not an “enhancement” can often get in the way of the proper ethical
questions: What are the good and bad uses of biotechnical power? What makes a
use “good,” or even just “acceptable”? It does not follow from the fact that a
drug is being taken solely to satisfy one’s desires—for example, to increase
concentration or sexual performance—that its use is objectionable. Conversely,
certain interventions to restore functioning wholeness—for example, to enable
postmenopausal women to bear children or sixty-year-old men to keep playing
professional ice hockey—might well be dubious uses of biotechnical power. The
human meaning and moral assessment must be tackled directly; they are unlikely
to be settled by the term “enhancement,” any more than they are by the nature
of the technological intervention itself.
VI. Beyond
Natural Limits: Dreams of Perfection and Happiness
Reliance on the therapy-versus-enhancement distinction has
one advantage in theory that turns out also to be a further disadvantage in
practice. The distinction rests on the assumption that there is a natural human
“whole” whose healthy functioning is the goal of therapeutic medicine. It sees
medicine, in fact, as thoroughly informed by this idea of health and wholeness,
taken as the end of the entire medical art. Medical practice, for the most part
and up to the present time, appears to embody this self-understanding of its mission.
Yet this observation points to the deepest reason why the distinction between
healing and enhancing is, finally, of insufficient ethical, and even less
practical, value. For the human being whose wholeness or healing is sought or
accomplished by biomedical therapy is finite and frail, medicine or no
medicine.
The healthy body declines and its parts wear out. The sound
mind slows down and has trouble remembering things. The soul has aspirations
beyond what even a healthy body can realize, and it becomes weary from
frustration. Even at its fittest, the fatigable and limited human body rarely
carries out flawlessly even the ordinary desires of the soul. For this reason
(among others), the desires of many human beings—for more, for better, for the
unlimited, or even for the merely different—will not be satisfied with the
average, nor will they take their bearings from the distinction between normal
and abnormal, or even between the healthy and the better-than-healthy.
Joining aspirations to overcome common human limitations
are comparable aspirations to overcome individual shortfalls in native
endowment. For there is wide variation in the natural gifts with which each of
us is endowed: some are born with perfect pitch, others are born tone-deaf;
some have flypaper memories, others forget immediately what they have just
learned. And as with talents, so too with desires and temperaments: some crave
immortal fame, others merely comfortable preservation. Some are sanguine,
others phlegmatic, still others bilious or melancholic. When nature dispenses
her gifts, some receive only at the end of the line. Yet, one should remember
that it is often the most gifted and ambitious who most resent their human
limitations: Achilles was willing to destroy everything around him, so little
could he stomach that he was but a heel short of immortality.
As a result of these infirmities, particular and universal,
human beings have long dreamed of overcoming limitations of body and soul, in
particular the limitations of bodily decay, psychic distress, and the
frustration of human aspiration. Dreams of human perfection—and the terrible
consequences of pursuing it at all costs—are the themes of Greek tragedy, as
well as of “The Birth-mark,” the Hawthorne short story with which the President’s
Council on Bioethics began its work. Until now these dreams have been pure
fantasies, and those who pursued them came crashing down in disaster. But the
stupendous successes over the past century in all areas of technology, and
especially in medicine, have revived the ancient dreams of human perfection.
Like Achilles, many of the major beneficiaries of modern medicine seem, by and
large, neither grateful nor satisfied with the bounties we have received from
existing biomedical technologies. We seem, in fact, less content than we are “worried
well,” perhaps more aware of hidden ills we might be heir to, or more worried
about losing the health we have than we are pleased to have it. Curiously, we
may even be more afraid of death than our forebears, who lived before modern
medicine began successfully to do battle with it. Unconsciously, but clearly as
a result of what we have been given, our desires grow fat for still further
gifts. And we regard our remaining limitations with less equanimity, to the
point that dreams of getting rid of them can be turned into moral imperatives.vi
For these reasons, thanks to biomedical technology, people will be increasingly
tempted to try to realize these dreams, at least to some extent: ageless and
ever-vigorous bodies, happy (or at least not unhappy) souls, excellent human
achievement (with diminished effort or toil), and better endowed and more
accomplished children. These dreams have at bottom nothing to do with medicine,
other than the fact that it is doctors who will wield the tools that may get
them realized. They are, therefore, only accidentally dreams “beyond therapy.”
They are dreams, in principle and in the limit, of human perfection.
Not everyone interested in the beyond-therapy uses of
biotechnology will dream of human perfection. Many people are more or less
satisfied, at least for now, with their native human capacities, though they
might willingly accept assistance that would make them prettier, stronger, or
smarter. The pursuit of happiness and self-esteem—the satisfaction of one’s
personal desires and recognition of one’s personal worth—are much more common
human aspirations than the self-conscious quest for perfection. Indeed, the
desire for happiness and the love of excellence are, at first glance,
independent aspirations. Although happiness is arguably fuller and deeper when
rooted in excellent activity, the pursuit of happiness is often undertaken
without any regard for excellence or virtue. Many people crave only some extra
boost on the path to success; many people seek only to feel better about
themselves. Although less radical than the quest for “perfection,” the quests
for happiness, success, and self-esteem, especially in our society, may prove
to be more powerful motives for an interest in using biotechnical power for
purposes that lie “beyond therapy.” Thus, though some visionaries—beginning
with Descartes—may dream of using biotechnologies to perfect human nature, and
though many of us might welcome biotechnical assistance in improving our native
powers of mind and body, many more people will probably turn to it in search of
advancement, contentment, and self-satisfaction—for themselves and for their children.
Why should anyone be worried about these prospects? What
could be wrong with efforts to improve upon or perfect human nature, to try,
with the help of biomedical technology, to gain better children, higher
achievements, ageless bodies, or happy souls? What are the sources of our
disquiet?
The answers to these questions cannot be given in the
abstract. They will depend on a case-by-case analysis, with special attention
to the ends pursued and the means used to pursue them. In some cases, disquiet attaches
not only to the individual pursuit of a particular goal, but also to the social
consequences that would follow if many people did likewise (for example,
selecting the sex of offspring, if practiced widely, could greatly alter a
society’s sex ratio). In other cases, disquiet attaches mainly to the
individual practice itself (for example, drugs that would erase or transform
one’s memories). Speaking in the abstract and merely for the sake of
illustration, concerns can and have been raised about the safety of the
techniques used and about whether access to the benefits will be fairly
distributed. Regarding the use of performance-enhancing techniques, especially
in competitive activities, concerns can be raised about unfair advantage and
inauthentic performance. Questions can be raised about coercion, overt and
subtle (through peer pressure), should uses of mind-improving drugs become
widespread. Other worries include the misuse of society’s precious medical
resources, the increasing medicalization of human activities, the manipulation
of desires, the possible hubris in trying to improve upon human nature, and the
consequences for character of getting results “the easy way” through
biotechnology, without proper effort or discipline. There is no point here in
detailing these further or in indicating additional possible objections. As
concerns arise in their appropriate contexts, we shall discuss them further. At
the end of this report, we will offer what generalizations seem appropriate.
Between now and then, we shall proceed to examine several instances of
activities and uses of biotechnical power that look “beyond therapy.”
VII. Structure
of the Inquiry: The Primacy of Human Aspirations
We have considered several different ways to organize our
inquiry. We could begin from the novel techniques: genetic screening,
gene insertion, or one or another of the various psychotropic drugs. We could
begin with the new powers or capacities these techniques provide:
to select the sex (or other traits) of offspring, to influence mood or memory,
or to alter the rate of biological aging. We could begin with the therapeutic
uses these powers might serve—for example, to treat depression or
dwarfism—and look next for the enhancement uses that lie beyond therapy. We
could begin with those aspects of human life that might be affected: our
inborn bodily or psychic capacities, our bodily or psychic activities, or the
phases and shape of the life cycle—how we are born, how we die, and how we live
in the prime of life. Or we could begin with the desires and goals that
either drive our pursuit of these techniques or that will enlist the available
powers they make possible once they are available: desires for longer life,
finer looks, stronger bodies, sharper minds, better performance, and happier
souls—in short, with our specific aspirations to improve our lot, our
activities, or the hand that nature dealt to us or to our children.
In keeping with our goal of “a richer bioethics”—one that
seeks to do justice to the full human meaning of biotechnological advance—we
will here proceed in the last of these ways. By structuring the inquiry around
the desires and goals of human beings, we adopt the perspective of human
experience and human aspiration, rather than the perspective of technique and
power. By beginning with long-standing and worthy human desires, we avoid
premature adverse judgment on using biotechnologies to help satisfy them. We
can also see better how the new technological possibilities for going “beyond
therapy” fit with previous and present human pursuits and aspirations,
including those well represented in the goals of modern medicine. We will also
be able critically to assess the desirability of these goals and the
significance of any successes in attaining them. What might the successful
pursuit of these goals—longer life, stronger bodies, happier souls, superior
performance, better children—using biotechnological means do to both the users
and the rest of society? Why might these consequences matter?
In Chapter Two,
we consider the pursuit of “better children,” using techniques of genetic
screening and selection to improve their native endowments or drugs that might
make them more accomplished, attentive, or docile. In Chapter
Three, we consider the pursuit of “superior performance,” using genetic or
pharmacologic enhancement, taking the domain of athletics as a specially
revealing instance. In Chapter
Four, we consider the pursuit of “ageless bodies,” both modest and bold,
using either soon-to-be-available genetic interventions to increase the strength
and vigor of muscles, or various efforts, somewhat more futuristic, to retard
the general processes of biological senescence. In Chapter
Five, we consider the pursuit of “happy (or satisfied) souls,” using
pharmacologic agents that dull painful memories or that brighten mood. In a
final chapter we briefly try to put together what we have learned from the
various “case studies.” While each of the separate instances will make our
concerns concrete, the full value of the inquiry requires considering all
these instances together and seeing them as part of a larger human
project—toward perfection and happiness.
VIII. Method
And Spirit
We conclude this introduction with a few words about the
method and spirit of our inquiry. In preparing ourselves for the analysis of
the various topics comprising the four middle chapters, we commissioned
presentations from a wide array of scientists working or writing in the
pertinent fields of biology and biotechnology: preimplantation genetic
diagnosis and genetic enhancement (Gerald Schatten
and Francis
Collins); choosing sex of children Arthur Haney
and Nicholas
Eberstadt); drugs to modify behavior in children ((Lawrence Diller
and Steven
Hyman); genetic enhancement of muscle strength and vigor (H. Lee Sweeney);
genetic enhancement of athletic performance (Theodore
Friedmann); aging and longevity research (Steven Austad
and S. Jay
Olshansky); memory, and drugs that might improve or blunt it (James McGaugh
and Daniel
Schacter); and mood-brightening drugs (Peter Kramer
and Carl
Elliott). Drawing on these presentations and on outside reading in the
various areas, Council staff prepared working papers on nearly all these
topics, and these papers were discussed at some length at eight Council
meetings between July 2002 and July 2003. Several Council Members contributed
original writings (Michael Sandel
on superior performance,Gilbert
Meilaender on memory, Paul McHugh on “medicalization,” Leon Kass on the
pursuit of perfection).6
The final report is the product of drafting by Council staff, reviewed and
critiqued by all Members of the Council, and rewritten many times.
The final document is not a research report, but an ethical
inquiry. It makes no pretense of comprehensiveness; it does not report
exhaustively on the literature, scientific or ethical. Rather, it aspires to
thoughtful reflection and represents mainly a (partial) distillation of the
Council’s own thinking. Not every Member shares every concern here expressed.
Different Members care more about different topics. All of us are aware that
there are issues not addressed and viewpoints not reflected. Yet, as a Council,
we own the document as a whole, offering it as a guide to further thinking on
this potentially very important topic.
Each of the four specialized chapters opens with a brief
but critical exploration of the goal under consideration (for example, what are
“better children” or “happy souls”). In due course we introduce the relevant
biotechnologies and the powers they provide for pursuing these goals. We then
proceed with our ethical analysis, trying to assess the meaning and possible
consequences of pursuing those goals by these means, and considering the
implications both for the individuals involved and for the broader society.
Because much of what lies “beyond therapy” lies also in the future, our
analysis is necessarily speculative, and by raising possible concerns we do not
mean to be setting ourselves up as prophets. As we readily acknowledge, which,
if any, of our speculative suggestions regarding possible future consequences
turn out to be correct will be a matter, in part, for careful empirical
research. At the same time, however, we also insist that figuring out which of
them will become a reality is not exactly the main point. Far more important,
in our opinion, the human goods and principles discussed here can help shape
our thinking across the entire range of technological powers (and the attendant
ethical dilemmas) that we are likely to face in the future. By raising the
questions we do, and by introducing certain matters of possible concern, we
seek to identify exactly the sorts of questions and concerns to which
researchers, policy makers, and the public at large should be paying attention.
The spirit of this inquiry is educational. In the first
instance, we want to help people sort out fact from fiction, real
biotechnological possibilities from merely imaginary ones. We want to clarify
the ethical and social issues, both for individuals and the larger society.
Precisely because we are taking a long-range view, we are primarily interested
in opening up questions, not in issuing moral pronouncements or suggesting
legislative or regulatory measures. Our first questions are not “Is this good
or bad, right or wrong?” or “Should we allow it?” but rather, “What does and
will this mean for us—as individuals, as members of American society, and as
human beings eager to live well in an age of biotechnology?” If the questions
we raise and the observations we offer strike the reader as conveying a
cautionary note, he or she should not mistake this for hostility to
biotechnology in general or to its many clearly desirable uses. Neither should
anyone be surprised by our concern. The benefits from biomedical progress are
clear and powerful. The hazards are less well appreciated, precisely because
they are attached to an enterprise we all cherish and support and to goals
nearly all of us desire. All the more reason to try to articulate the human
goods that we seek to defend and the possible threats they may face.
_________________
Footnotes
i.These range from “engineering and biological study of
relationships between human beings and machines” (Webster’s II New Riverside
University Dictionary, 1988), to “biological science when applied
especially in genetic engineering and recombinant DNA technology” (Merriam-Webster
OnLine Dictionary, 2003), to “the use of biological processes to solve
problems or make useful products” (Glossary provided by BIO, the Biotechnology
Industry Organization, www.bio.org, 2003). In the broader sense of the term
that we will follow here, older biotechnologies would include fermentation
(used to bake bread and brew beer) and plant and animal hybridization. Newer
biotechnologies would include, among others, processes to produce genetically
engineered crops, to repair genetic defects using genomic knowledge, to develop
new drugs based on knowledge of biochemistry or molecular biology, and to
improve biological capacities using nanotechnology. They include also the
products obtained by these processes: nucleic acids and proteins, drugs,
genetically modified cells, tissues derived from stem cells, biomechanical
devices, etc.—in short, any industrially developed, useful agent that can alter
the workings of the body or mind.
ii.The importance, for assessing biomedical technologies,
of the distinction between (1) the techniques and (2) the powers they make
available was first developed nearly thirty years ago in a report from the
National Research Council/National Academy of Sciences, Assessing Biomedical
Technologies: An Inquiry into the Nature of the Process (Committee on Life
Sciences and Social Policy, National Academy of Sciences, Washington, D.C.,
1975). The report recommended (and illustrated by example) that assessment of
biomedical technologies concern itself with implications of both the techniques
and the perfected powers they provide. (See pages 1 and 9, and the structure of
the analysis in each chapter.) We generally prefer the more energetic word “power,”
with its implication of efficacy, to the more prosaic “capacity” or “ability,”
but we mean by it nothing ominous or sinister. As we use it, “power” is to be
understood as neutral or better, certainly when compared to its opposite, “impotence.”
At the same time, however, this term invites us to think about power’s misuse
or abuse; such reminders do not shadow the more quiescent near-synonyms, “capacity”
or “ability.”
iii. The already widely accepted “beyond therapy” uses of
biomedical technologies include: pills for sleep and wakefulness, weight loss,
hair growth, and birth control; surgery to remove fat and wrinkles, to shrink
thighs, and to enlarge breasts; and procedures to straighten teeth and select
the sex of offspring. These practices are already big business. In 2002
Americans spent roughly one billion dollars on drugs used to treat baldness,
about ten times the amount spent on scientific research to find a cure for
malaria, a disease that afflicts hundreds of millions of people worldwide.
iv. Our choice of “Beyond Therapy” as the title for this
report is meant to acknowledge that this notion offers a good point of entry:
it reflects the medical milieu in which the questions arise; it exposes the
untraditional goals of the new uses for biotechnical power; it hints at the
open-ended character of what lies “beyond” the goal of healing. Yet for reasons
that should become clear, the notion of “beyond therapy” does not seem to us to
define the royal road to understanding. For this, one must adopt an outlook not
only “beyond therapy” but also “beyond the distinction between therapy and
enhancement.” One needs to see the topic less in relation to medicine and its
purposes, and more in relation to human beings and their purposes.
v. According to the Oxford English Dictionary, “to
enhance,” means “to raise in degree, heighten, intensify”; “to make to appear
greater”; “to raise in price, value, importance, attractiveness, etc.” An “enhancement”
would designate a quantitative change, an increase in magnitude or degree.
vi. Consider in this connection our attitudes toward organ
transplantation. When first introduced into clinical practice some fifty years
ago, receiving a life-saving kidney transplant was regarded as a gift, a
blessing, a minor miracle, something beyond anything merited or even expected.
Today, though the number of such “miracles” increases annually, supply does not
equal demand. Expectations have risen to such an extent that people speak and
act as if society’s failure to meet the need is in fact the cause of death for
those who die before they can be transplanted. Who in 1950 could have thought
that he was entitled to have his defective and diseased organs replaced? Will
people in 2050 think that they are entitled to have any and all their weakened
parts replaced, and not just once?
Endnotes
1. National Science Foundation, Converging Technologies for Improving Human Performance: Nanotechnology, Biotechnology, Information Technology and Cognitive Science, Arlington, Virginia: National Science Foundation, 2003, p. 6.
2. Stock, G., Redesigning Humans: Our Inevitable Genetic
Future, New York: Houghton Mifflin, 2002, p. 200. A similar opinion has been
voiced by Lee Silver: “[W]e’re going to be able to manipulate and control the
genes that we give to our children. It’s just over the horizon. . . . All of
these new technologies are going to change humankind as we know it.” (“Frontline”
interview, www.pbs.org.) See also Silver, L., Remaking Eden: Cloning and
Beyond in a Brave New World, New York: Avon, 1998. Silver’s enthusiasm for
the post-human future is diluted only by his fear that not everyone will have
equal access to its enhancing benefits. For an examination and critique of
these views, see Fukuyama, F., Our Posthuman Future: Consequences of the
Biotechnology Revolution, New York: Farrar Straus & Giroux, 2002.
3. James D. Watson, quoted in Wheeler, T., “Miracle Molecule,
50 Years On,” Baltimore Sun, 4 February 2003, p. 8A. At a symposium in
Toronto in October 2002, Watson went further in his support of enhancement: “Going
for perfection was something I always thought you should do. You always want
the perfect girl.” (Abraham, C., “Gene Pioneer Urges Human Perfection,” Toronto
Globe and Mail, 26 October 2002.) The article further quotes Watson’s
response to the charge that he wants to use genetics “to produce pretty babies
or perfect people”: “What’s wrong with that?” he countered. “It’s as if there’s
something wrong with enhancements.”
4. Descartes, Discourse on the Method of Conducting One’s
Reason Well and Seeking Truth in the Sciences, Part VI, para. 2. Private
translation by Richard Kennington.
5. See, for example, Parens, E., ed., Enhancing Human
Traits, Washington, D.C.: Georgetown University Press, 1998; and Elliott,
C., Better Than Well: American Medicine Meets the American Dream, New
York: Norton, 2003.
6. The transcripts of all the presentations and Council
discussions, as well as the texts of the staff working papers and the papers
written by Members, are available on the Council’s website: www.bioethics.gov.
==============================
Chapter 2. Better Children
What father or mother does not dream of a good life for his
or her child? What parents would not wish to enhance the life of their
children, to make them better people, to help them live better lives? Such
wishes and intentions guide much of what all parents do for and to their
children. To help our children on their way and to make them strong in body and
in mind, we feed and clothe them, see that they get rest, fresh air, and
exercise, and take great pains regarding their education. Beyond ordinary
schooling, we give them swimming and piano lessons, enroll them in Scouts or
Little League, and help them acquire a variety of skills—artistic,
intellectual, and social. In addition, we try to develop their character,
educate their tastes and sensibilities, and nurture their spiritual growth. In
all of these efforts we are guided, whether consciously or not, by some notion
or other of what it means to improve our children, of what it means to
make them better.
Needless to say, the thing is easier said than done.
Rearing children is work only for the brave. Children can be recalcitrant,
outside influences can corrupt, and even the best of efforts may not bear good
fruit. But even apart from the practical difficulties, the very aspiration of “producing
better children” is hardly trouble-free, even for parents and teachers with the
best of intentions. For it is easier to wish whole-heartedly that our
children be improved than it is to know what that would mean. For what,
exactly, is a good or a better child?
Is it a child who is more able and talented? If so, able in
what and talented how? Is it a child with better character? If so, having which
traits or virtues? More obedient or more independent? More sensitive or more
enduring? More daring or more measured? Better behaved or more assertive? Is it
a child with the right attitude and disposition toward the world? If so, should
he or she tend more toward reverence or skepticism, high-mindedness or toleration,
the love of justice or the love of mercy? As these questions make clear, human
goods and good humans come in many forms, and the various goods and virtues are
often in tension with one another. Should we therefore aim at balanced and “well-rounded”
children, or should we aim also or instead at genuine excellence in some one or
a few dimensions? It is not easy to answer. Yet absent knowledge regarding
these matters, acting on the laudable intention of producing better children
can be a tricky, not to say dangerous, business.
This is especially true because of a second difficulty, one
derived not from the ambiguity of “good” or “better” but from the ambiguity
that is at the heart of being a child. Children much more than adults
are, so to speak, double creatures: they are both who they are here-and-now
and, at the same time, they are also creatures on the way to maturity and
adulthood. To be a child means “to-be-not-yet,” means to be “on-the-way-up,”
growing up, maturing, reaching toward one’s prime. Yet to be a child is also to
enjoy a special time of our lives, with special gifts, possibilities, and
opportunities, and—in comparison with adulthood—with a relatively carefree
existence. Childhood is that stage of life justly celebrated as most innocent,
open, fresh, playful, wondering, unself-conscious, spontaneous, and honest: “out
of the mouths of babes.” This “doubleness” of childhood is responsible for the
notorious paradox of parenthood: we love our children unconditionally, just as
they are, yet we are constantly doing everything in our power to get them to be
different, to change for the better. Not content just to appreciate them in
their childish glory, we labor to educate them, to lead them out of childhood,
and to draw from them those latent but still largely dormant powers and virtues
they do not as yet have or have not yet expressed. The task is made still more
paradoxical once we remember the most important improvement we seek to promote:
their ability to do without our educative meddling, to take the reins of their
own chariots, and, in the best case, to repay the debt they owe us by doing the
same for the next generation.
This delicate process of rearing the young, supporting and
savoring them as they are while coaxing and directing them toward what they
might well become, requires special attention to the means of improvement. As
hard as it may be to say with confidence what we mean by “a better
child,” it is equally difficult to select the proper means. Even were we
to agree that it were desirable that our children be well-behaved, excellent in
their studies, or able to handle disappointment, there are tough questions
about which means are best suited to these ends. The use of some means might
actually undermine the goal, especially if they achieve their effect without
demanding effort or engagement of the child himself; having a child do his
arithmetic homework with a calculator will get him the right answers without
teaching him long division. Also, the availability of new and attractive means
that facilitate one-sided pursuits of a partial goal (for example, superior
athletic or academic performance) can threaten the overall goal of rearing: to
enable our children to flourish as autonomous adults who can think and act for
themselves, learn from adversity, and meet life’s vicissitudes with resilience
and self-confidence.
These enduring perplexities regarding our aspiration for
better children now deserve our thematic and heightened attention. The reason:
new biotechnologies, present and projected, are providing new and allegedly
powerful means for improving our children. Thinking about these possibilities
invites us to examine our existing practices and purposes, even as we try to
figure out what is new and how it matters.
In most of our efforts to assist our children’s
development, we proceed through speech and symbolic deed, using praise and
blame, reward and punishment, encouragement and admonition, as well as
habituation, training, and ritualized activities. Yet nature sets limits on
what can be accomplished by education and training alone. No matter how much we
try to help, the tone-deaf will need more training to learn to carry a tune,
the short will be less likely to excel at basketball, the irascible will have
trouble restraining their tempers, and the insufficiently smart will remain
handicapped for competitive college admissions. If the inborn “equipment” is
faulty, or even only normally limited and hence inadequate for realizing some
human purposes, it is inviting to think about improving the native powers or
the efficacy of their expression and use. For whether we like it or not,
certain desired improvements in our children will be possible, if at all, only
by improving their native equipment.
Even before the coming of the present age of biotechnology,
we have used technological adjuncts to improve upon nature’s gifts. We give our
children supplementary vitamins, fluoridated toothpaste, and, where necessary,
corrective lenses or hearing aids. We even use biological means of improving
their limited human capacity to resist disease: we immunize our children
against polio, diphtheria, and measles, among other infectious diseases, by
injecting them with attenuated viruses and bacteria in the form of vaccines.
But the scope of these now-routine kinds of biomedical improvement has until
now been limited to restoring or protecting our children’s health in a quite
straightforward sense.
It is here where some truly novel biotechnologies enter the
picture. According to some predictions, our ability to improve our children’s
native endowments may soon take a quantum leap, thanks to prospects for
genetically engineered improvements of native human powers and drug-assisted
improvements in their use. It is these prospects—for so-called “designer babies”
and for drug-enhanced children—that we shall consider in the present chapter.
The technologies differ widely, so that they are rarely considered together.
Yet once seen in the context of the common goal, “better children,” they raise
overlapping and similarly profound ethical and social issues—especially about
the significance of procreation, the nature of parental responsibility, and the
meaning of childhood.
I. Improving
Native Powers:
Genetic Knowledge and Technology
A. An Overview
The possibility of using genetic knowledge and genetic
engineering to improve the human race and its individual members has been
discussed for many years, especially in the heady decades immediately following
Watson and Crick’s discovery, in 1953, of the structure of DNA. New life was
breathed into old eugenic dreams, which had been temporarily discredited by the
Nazi pursuits of a “superior race.” As late as the early 1970s, serious
scientists talked optimistically about humankind’s new opportunity to take the
reins of its own evolution, thanks to the predicted confluence of genetic
engineering and reproductive technologies.1
But as scientists have learned just how difficult it is to engineer precise
genetic change—even to treat individuals with genetic diseases caused by a
simple one-gene mutation—explicit talk about improving the species has largely
faded. Instead recent years have seen, in its place, much talk about coming
prospects for “designer babies,” children born with improved genetic
endowments, the result either of careful screening and selecting of embryos
carrying desirable genes, or of directed genetic change (“genetic engineering”)
in gametes or embryos.
Interest in such possibilities has been fueled by recent
developments in a number of related disciplines, beginning with the completion
of the Human Genome Project. Knowledge of the complete chemical sequence of all
human genes promises greatly increased powers for genetic screening of
individuals and embryos. Numerous studies are already seeking to correlate
phenotypic traits (and not only those connected with disease) with the presence
or absence of certain genetic markers. Scientists have reported early success
with directed genetic change in embryos of non-human animals (including
primates2),
though many more attempts have failed. And we are witnessing large increases in
the use of assisted reproductive technologies, including for purposes that go
beyond the mere treatment of infertility.3
Extrapolating from these developments, some scientists have predicted that
parents, in the not-too-distant future, will be able to exert precise genetic
control over many characteristics of their offspring.4
These predictions have been greeted both with enthusiasm—”At last, we can
escape from the tyranny of fortune and bring our inheritance under rational
control!”—and with alarm—”What hubris! Scientists are trying to play God!”
It is difficult to know what to make of these predictions,
based as they are largely on speculation. In this enormously fertile and
rapidly developing field, the future is unknowable. Thus, anyone can claim to
be a prophet, and no one should confidently bet against any form of scientific and
technological progress. Yet in our view, for reasons that we shall elaborate
below, prophecies and predictions of a “new (positive) eugenics” seem greatly
exaggerated. In consequence, much of the public disquiet created by loose talk
of genetically engineered “designer babies” seems unwarranted. Nevertheless,
the public’s misgivings may contain a partial wisdom regarding practices in
this area that are not far-fetched, indeed, that are already with us, including
prenatal and preimplantation genetic screening. For, as we shall see, there is
some reason to be concerned both about negative eugenics and about the practice
of genetic selection of “better” children. Therefore, even as we try to
calm down fears about genetic engineering of children, it behooves us to pay
careful attention to the reasons behind them and to the human goods at stake.
By this means, we may shed light on the meaning not only of things we might be
doing in the future but also of things we are already doing in the present.
B. Technical Possibilities
One can distinguish several ways of trying to produce
children with better genetic endowments. First is the use of directed mating,
either choosing “superior” mating partners or using donor sperm or donor eggs
(or both) obtained from “superior” individuals. Assuming that people with some
superior natural ability or accomplishment are genetically better endowed, and,
further, that such putative genetic excellence is heritable, directed mating of
like with like, so the theory goes, would increase the odds of getting superior
children. People seeking to initiate a pregnancy using artificial insemination
by donor (AID) or in vitro fertilization (IVF) with donor eggs do check the
pedigree (and will soon be able to check the genetic profile) of the prospective
donor for general health and fitness, as well as for certain desired traits,
from height and hair color to intelligence. In some notorious cases, people
planning to undergo IVF have advertised in elite college newspapers, offering
up to $100,000 for an egg donor with high SAT scores or “proven college-level
athletic ability.”5
Yet these approaches to genetic improvement are relatively crude and probably
unreliable, since they all involve the uncertain lottery of chance inherent in
all sexual reproduction, and they overestimate the degree to which heredity by
itself determines traits such as intelligence or athletic ability. Moreover,
most couples would rather have their own children than those they might get by
using gametes from a “superior” donor.i
We will not be discussing this approach further.
We concentrate instead on various powers that depend upon
precise genetic knowledge and technique: (a) the ability to screen and select
fetuses, embryos, and gametes (egg and sperm) for the presence or absence of
specific genetic markers; and (b) the ability to obtain and introduce such
genetic material in order to effect a desired genetic “improvement.” The first,
by itself, leads to two powers that merely select from among genetic endowments
conferred by chance, the difference between them being the stage at which
screening is done and whether selection is “negative” or “positive.” Prenatal
diagnosis during an established pregnancy (using amniocentesis or chorionic
villus sampling) permits the weeding out, through abortion, of those fetuses
carrying undesired genetic traits.ii
Preimplantation genetic screening and selection of in vitro embryos, in
contrast, permits pregnancy to begin using only those embryos that carry desired
genetic traits.iiii
In contrast to both of these, a third power, directed genetic change (or
genetic engineering), would attempt to go beyond what chance alone has
provided, improving in vitro embryos directly by introducing “better” genes.iv
In theory, these three prospects offer scientists and
prospective parents a range of increasing genetic control, from (1) eliminating
the bad (“screening out”), through (2) selecting the good (“choosing in”), to
(3) redesigning for the better (“fixing up”). Each activity raises its own
ethical questions, some of which we shall consider later. But in practice, they
are not equally feasible as means of producing better children, and, for
reasons discussed below, we believe that the scale of their use for this
purpose will probably remain low.
We state the conclusion in advance: The first, prenatal
diagnosis and selective abortion, widely practiced since the 1970s in order to
prevent the birth of children with genetic or chromosomal abnormalities, is a
weeding-out procedure; hence its potential to select “better than normal”
babies is negligible, and it is unlikely ever to be effective or widely used
for such purposes.v
The third and most ambitious, genetic engineering of improved children,
is—contrary to much loose prediction—a most unlikely prospect, for reasons of
both feasibility and safety. The second, selecting IVF embryos genetically
predisposed to certain superior or desirable traits, might soon be possible for
some relatively uncomplicated traits (for example, height or leanness). Yet
even here, as we shall see, there will likely be large—perhaps
insurmountable—logistical problems in obtaining a “genetically superior” embryo
for any trait to which many different genes contribute. Moreover, absent
certain innovations in technology (and greater insurance coverage for assisted
reproduction procedures), this is unlikely to be a widespread practice in the
near future, save for those who are willing and able to undergo IVF and to pay
extra for the genetic screening. Finally, keeping in mind that most traits of
interest to parents seeking better children are heavily influenced by
environment, even successful genetic screening and embryo selection might not,
in many cases, produce the desired result.
We look briefly at each of the alternatives.
1. Prenatal Diagnosis and Screening Out.
Genetic screening by amniocentesis or chorionic villus
sampling is an established feature of prenatal care in the United States and
other economically advanced countries. It is routinely offered to women of
advanced maternal age or to parents known to be carriers of heritable
disorders. Some prospective parents prefer not to screen and not to know, in
many cases because they have decided that they will not abort, no matter what.
But the use of the practice is growing, and it will in all likelihood continue
to do so. The capacity for screening both parents-to-be and fetuses is certain
to increase, thanks to the completed mapping of the human genome and to greatly
improved efficiency of testing. In addition to detecting more genetic diseases,
new screening powers may also be able to detect a growing number of genetic
markers that correlate statistically with the presence (or absence) of certain
heritable—and desirable—traits (for example, tallness, leanness, perfect pitch,
longevity, and perhaps even temperament and eventually intelligence). For
parents willing to abort and try again repeatedly, prenatal screening could in
principle be used to try to land a “better”—and not just a disease-free—baby.
But, in practice, such an approach—even leaving ethical issues aside—is
unfeasible on scientific grounds. No genetic selection can “optimize” beyond
what the parents have contributed to the fetus. Moreover, an enormous number of
“trial pregnancies” would be needed to get an “optimum baby” for any polygenic
trait. For all these reasons this entire approach strikes us as far-fetched,
and we shall not consider it further as a realistic possibility.
Yet, before leaving this subject, we think it important to
observe that the existence and normalization of prenatal diagnosis and abortion
for genetic defect have already had significant effects on our thinking: about
our genetic endowments, about reproductive choice and responsible parenthood,
and about what constitutes a good or “good enough” child. Attitudes and
opinions acquired in connection with this practice will certainly influence how
we are likely to think about and deal with the coming new techniques for
selecting or altering our prospective children. The ethical issues will be
discussed in greater detail later, in the section devoted to them. To prepare
that discussion, it is worth noting a few salient facts about the current
practice of prenatal diagnosis and some of its social implications—regarding
medicine, children, and parental prerogative and responsibility.
First, prenatal diagnosis has enabled many couples to avoid
the sorrows and burdens of rearing children with severe genetic and chromosomal
disorders. Anyone who has been close to families having children with Tay-Sachs
disease or anencephaly knows the anguish and misery that are now preventable by
such means. Children born with these and comparable abnormalities endure
serious and lifelong physical and mental disabilities. With certain of the conditions,
postnatal care can restore some hope of a normal life; with others, such care
is moderately palliative at best, and the children afflicted by these diseases
are often destined to live relatively short lives marked by persistent physical
pain and profound mental retardation. Without the option of prenatal screening,
many couples at high risk for such genetic abnormalities would choose not to
bear children at all; prenatal screening has also enabled women who have
already given birth to an affected child or who are past the age of thirty-five
(when the risk of chromosomal abnormalities begins to rise sharply) to become
pregnant with some confidence of bearing healthy children.
Yet, second, to achieve these benefits prenatal diagnosis
adopts a novel approach to preventive medicine: it works by eliminating the
prospective patient before he can be born. This kind of preventive medicine is
thus in fact a species of negative eugenics—elimination of the genetically
unfit and a reduction in the incidence of their genes—albeit carried out
voluntarily and on a case-by-case basis. It is true that the tests themselves
are value-neutral and that many genetic counselors are committed to
non-directive counseling, leaving prospective parents free to exercise their individual
choices based on their own value judgments. Yet the very availability of these
tests—accompanied in many cases by subtle pressures, applied by counselors (and
others) to prospective parents, to abort any abnormal fetus—strongly implies
that certain traits are or should be disqualifying qualities of life that
justify prevention of birth.
Third, the practice of prenatal screening has established
as a cultural norm (or at least as a culturally acceptable norm) a new notion
about children: the notion that admission to life is no longer unconditional,
that certain conditions or traits are disqualifying. To be sure, parents
confronted with the painful decision whether or not to abort an affected fetus
may feel deeply divided and moved by considerations on both sides of the issue,
but there appears to be a growing consensus, both in the medical community and
in society at large, that a child-to-be should meet a certain (for now,
minimal) standard to be entitled to be born. Although, at least in the United States,
the practice of screening and elimination is likely to remain voluntary, its
growing use could have subtly coercive consequences for prospective parents and
could increase discrimination against the “unfit.” Children born with defects
that could have been diagnosed in utero may no longer be looked upon as “Nature’s
mistakes” but as parental failings.
Finally, the practice of prenatal screening establishes the
principle that parents may choose the qualities of their children, and choose
them on the basis of genetic knowledge. This new principle, in conjunction with
the cultural norm just mentioned, may already be shifting parental and societal
attitudes toward prospective children: from simple acceptance to judgment and
control, from seeing a child as an unconditionally welcome gift to seeing him
as a conditionally acceptable product. If so, these changes in attitude might
well carry over beyond choices confined to the presence or absence of genetic
diseases, to the presence or absence of other desired qualities. Far from
producing contentment and gratitude in the parents, such changes might feed the
desire for better—and still better—children.
2. Genetic Engineering of Desired Traits (“Fixing Up”).
With directed genetic change aimed at producing certain
desired improvements, we enter the futuristic realm of “designer babies.”
Proponents have made this prospect look straightforward, and, on a theory of
strict genetic determinism, it is. One would first need to identify all (or
enough) of the specific variants of genes whose presence (or absence)
correlates with certain desired traits: higher intelligence, better memory,
perfect pitch, calmer temperament, sunnier disposition, greater ambitiousness,
etc. Once identified, the requisite genes could be isolated, replicated or
synthesized, and then inserted into the early embryo (or perhaps into the egg
or sperm) in ways that would eventually contribute to the desired phenotypic
traits. In the limit, there is talk of babies “made to order,” embodying a slew
of desirable qualities acquired with such genetic engineering. But in our
considered judgment, these dreams of fully designed babies, based on directed
genetic change, are for the foreseeable future pure fantasies. There are huge
obstacles, both to accurate knowing and to effective doing. One of these
obstacles—the reality that these traits are heavily influenced by
environment—will not be overcome by better technology.
Most of the traits for which parents might wish to engineer
improvements in their children—appearance, intelligence, memory—are most
certainly polygenic, that is, traits (or phenotypes) that depend on specific
genes or their variants at several, perhaps many, distinct loci. In such cases
the relationships and interactions among these genes (and between one’s genes
and the environment) are certain to be enormously complex.vi
Isolating all the relevant genetic variants, and knowing how to work with them
to produce the desired result, will therefore prove immensely difficult. To be
sure, not every trait for which parents might wish to select need turn out to
be highly polygenic: for example, height, skin color, eye color, or even the
genetic contributions to sexual orientation or basic temperament might be
heavily influenced by a very few genes. As we will see more fully in Chapter
Four, one mutation in a single gene has been shown to result in enormous
increases in the lifespan of flies, worms, and mice, and the same gene has been
identified in humans. Yet even here there would be no guarantee that the
predisposing genes, even if correctly and safely introduced into the zygote or
early embryo, would necessarily express themselves as desired, to yield the sought-for
improvement.
Even more of an obstacle to successful genetic engineering
is the practical difficulty of inserting genes into embryos (or gametes) in
ways that would produce the desired result and only the desired result.
Getting the genes into the right place in the cell, able to function yet
without disturbing regular cellular functions, is an enormously challenging
task. Insertion of genes into the host genome can cause abnormalities, either
by activating harmful genes or by inactivating useful ones. Recently, for
example, children undergoing experimental gene therapy for immune system
deficiencies have developed leukemia after retroviral gene transfer into bone
marrow stem cells, very likely the result of activation of a cancer-producing
gene by the virus used to transfer the therapeutic genes into the cell.6
And should introduced genes become inserted into inappropriate locations,
normal host genes could be inactivated. Moreover, because many genes are
pleiotropic—that is, they influence many traits, not just one—even a properly
inserted gene introduced to enhance a particular trait would often have
multiple effects, not all of them for the better.
Running such risks might be justified in gene therapy
efforts for already existing individuals, where the genes hold out the only
hope of cure for an otherwise deadly disease. But these safety risks will pose
formidable obstacles to all interventions in gametes or embryos, especially nontherapeutic
interventions aimed at producing children who would allegedly be, in one
respect or another, “better than well.” It is difficult to see how such an
intervention could ever be considered ethical, especially since the negative
effects might extend to future generations.
As a possible way around the hazards of gene insertion,
some researchers have proposed the assembly and injection of artificial
chromosomes: the new “better” genes could be packaged in small, manufactured
chromosomal elements that, on introduction into cells, would not integrate into
any of the normal forty-six human chromosomes. Such artificial chromosomes
could, in theory, be introduced into ova or zygotes without fear of causing new
mutations. But methods would have to be found to guarantee the synchronized
replication and normal segregation of such artificial chromosomes. Otherwise,
the package of improved genes, once introduced into the embryo, would not be
conserved in all cells after normal mitotic division. Even more dauntingly, any
gene introduced on such a chromosome would now be present in three copies (one
from mother, one from father, and one on the extra chromosome) instead of the
usual two, throwing off the normal balance of gene copies among all the genes.
The consequences of such “triploidy” can be deleterious (for example, Down
syndrome). All in all, safety and efficacy standards would seem to preclude
doing such experiments with human subjects, at least in the United States, for
the foreseeable future.vii
It is true that research along these lines might be undertaken in other
countries (for example, China), by scientists unconstrained by these
considerations, with eventual success in effecting directed genetic change in
human embryos. But, at least for the time being, we believe that we may set
this prospect safely to the side.
3. Selecting Embryos for Desired Traits (“Choosing In”).
Unlike the prospect for precise genetic engineering through
directed genetic change, the possibility of genetic enhancement of children
through embryo selection cannot be easily dismissed. This approach, less
radical or complete in its power to control, would not introduce new genes but
would merely select positively among those that occur naturally. It depends
absolutely on IVF, as augmented by the screening of the early embryos for the
presence (or absence) of the desired genetic markers, followed by the selective
transfer of those embryos that pass muster. This would amount to an “improvement-seeking”
extension of the recently developed practice of preimplantation genetic
diagnosis (PGD), now in growing use as a way to detect the presence or absence
of genetic or chromosomal abnormalities before the start of a pregnancy.
As currently practiced, PGD works as follows: Couples at
risk for having a child with a chromosomal or genetic disease undertake IVF to
permit embryo screening before transfer, obviating the need for later prenatal
diagnosis and possible abortion. A dozen or more eggs are fertilized and the
embryos are grown to the four-cell or the eight-to-ten-cell stage. One or two
of the embryonic cells (blastomeres) are removed for chromosomal analysis and
genetic testing. Using a technique called polymerase chain reaction to amplify
the tiny amount of DNA in the blastomere, researchers are able to detect the
presence of genes responsible for one or more genetic disorders.viii
Only the embryos free of the genetic or chromosomal determinants for the
disorders under scrutiny are made eligible for transfer to the woman to
initiate a pregnancy.
The use of IVF and PGD to move from disease avoidance to
baby improvement is conceptually simple, at least in terms of the techniques of
screening, and would require no change in the procedure. Indeed, PGD has
already been used to serve two goals unrelated to the health of the
child-to-be: to pre-select the sex of a child, and to produce a child who could
serve as a compatible bone-marrow or umbilical-cord-blood donor for a
desperately ill sibling. (In the former case, chromosomal analysis of the
blastomere identifies the embryo’s sex; in the latter case, genetic analysis
identifies which embryos are immunocompatible with the needy recipient.) It is
certainly likely that blastomere testing can be adapted to look for specific
genetic variants at any locus of the human genome. And even without
knowing the precise function of specific genes, statistical correlation of the
presence of certain genetic variants with certain phenotypic traits (say, with
an increase in IQ points or with perfect pitch) could lead to testing for these
genetic variants, with selection following on this basis. As Dr. Francis
Collins, director of the National Human Genome Research Institute, noted in his
presentation to the Council, the time may soon arrive in which PGD is practiced
for the purpose of selecting embryos with desired genotypes, even in the
absence of elevated risk of particular genetic disorders.7
Dr. Yury Verlinsky, director of the Reproductive Genetics Institute in Chicago,
has recently predicted that soon “there will be no IVF without PGD.”8
Over the years, more and more traits will presumably become identifiable with
the aid of PGD, including desirable genetic markers for intelligence,
musicality, and so on, as well as undesirable markers for obesity,
nearsightedness, color-blindness,ix
etc.
Yet, as Dr. Collins also pointed out to the Council, there
are numerous practical difficulties with this scenario. For one thing, neither
of the parents may carry the genetic variant they are most interested in
selecting for. Also, selecting for highly polygenic traits would require
screening a large number of embryos in order to find one that had the desirable
complement. With only a dozen or so embryos to choose from, it will not be
possible to optimize for the many necessary variants.x
The practice of PGD and selective transfer is still quite
new, and fewer than 10,000 children have been born with its aid. How likely or
widespread such a practice might become is difficult to predict. As we have
already indicated, a number of practical issues would need to be addressed
before PGD could be extended to permit selection of desirable traits beyond the
absence of genetic disorders. First are questions of possible harm caused by
removing blastomeres for testing (up to a sixth or even a quarter of the embryo’s
cells are taken). Although current evidence (from limited practice) suggests
that the procedure inflicts neither any immediately visible harm on the early
embryos, nor any obvious harm on the child that results, more attention to
long-term risks to the child born following PGD is needed before many people
would consider using it for “improvement” purposes only. Because many of the
desirable human phenotypic traits are very likely polygenic, the contribution
of any single gene identifiable by blastomere testing is likely to be small,
and the likelihood of finding all the “desired” genetic variants in a single
embryo is exponentially smaller still. Testing for multiple genetic variants
using the DNA from a single blastomere is likely to be limited—for a time—by
the quantities of DNA available, the sensitivity of the genetic tests, and the
ability to perform multiple tests on the same sample. But it seems only a
matter of time before techniques are perfected that will permit simultaneous
screening of IVF embryos for multiple genetic variants. And should some of the “desirable”
genes come grouped in clusters, selection for at least some desired traits
might well be possible.
Finally, even if PGD could be used successfully to select
an embryo with a number of desirable genetic variants, there is simply no
guarantee that the child born after this procedure would grow up with the
desired traits. The interplay of nature and nurture (genes and environment) in
human development is too complex and too little understood to make such results
predictable. Given that IVF combined with PGD is an inconvenient and expensive
alternative to normal procreation, and given that success is doubtful at best,
the purely elective use of this procedure seems unlikely to become widespread
in the foreseeable future. As Professor Steven Pinker put it, in his
presentation to the Council:
The choice that parents would face in a hypothetical future
in which even genetic enhancement were possible would not be the one that’s
popularly portrayed, namely, “Would you opt for a procedure that would give you
a happier, more talented child?” When you put it like that, well, who would say
no to that question? More realistically, the question that parents would face
would be something like this: “Would you opt for a traumatic and expensive
procedure that might give you a very slightly happier and more talented child,
might give you a less happy, less talented child, might give you a deformed
child, and probably would do nothing?”9
Nevertheless, we think it would be imprudent to ignore
completely this approach to “better children.” More and more people are turning
to assisted reproduction technologies (ART): in parts of western Europe,
roughly five percent of all births involve ART; in the United States, it is
roughly one percent and climbing, as the average maternal age of childbirth
keeps rising and family size keeps declining. More and more people are using
IVF not merely to overcome infertility but to screen and select embryos free of
certain genetic defects. Women who plan to delay childbearing are being
encouraged to consider early removal and cryopreservation of their own youthful
ovarian tissue, to be reintroduced into their bodies at sites easily accessible
for egg harvesting when they decide to have children. Other novel methods of
obtaining supplies of eggs for IVF—possibly including deriving them in bulk
from stem cells10—would
make the procedure less burdensome, and would, in theory, permit the creation
of a large enough population of embryos to make screening for polygenic traits
feasible.
The anticipated vast extension of genetic screening will
make many more couples aware of the risks they run in natural reproduction, and
they may choose to turn to IVF to reduce them—especially if obtaining eggs
became easy. Once more and more couples start screening embryos for
disease-related concerns, and once scientists have identified those genes that
correlate with various admirable traits, the anticipated expansion of improved
and more precise screening techniques might enable users of IVF to screen for “desirable
genes” as well. People already using PGD to screen for disease markers might
seek information also about other traits, as they have with sex or
histocompatibility. And if, once screening becomes automated, its cost comes
down, or if society decides to reimburse for PGD (regarding it as less
expensive than the care of genetically diseased children), the use of this
approach toward “better children” might well become the practice of at least a
significant minority. Under these circumstances, should genuine and significant
improvements be achieved for a few highly desired attributes (say, in maximum
lifespan; see Chapter Four), one can easily imagine that there would be an
increased demand for the practice, inconvenient or not. In the meantime, we
would do well to consider the ethical implications not only of such future
prospects but also of our current practices that make use of genetic knowledge.
C. Ethical Analysis
The technologies we have just considered range from the
well-established (prenatal “screening out,” using amniocentesis and abortion)
to the speculative (embryonic “fixing up,” using direct genetic modification of
embryos or gametes), with special attention to the new and growing (“choosing
in,” using preimplantation genetic diagnosis followed by selective embryo
transfer). It bears emphasis that genetic technologies have been and are being
devised mainly with the intention of producing healthier children—not “enhanced
children” or “super-babies,” but children who are better only in the sense of
being free of severe disease and deformity. As we have suggested, we have our
doubts whether these powers will soon be widely employed for any other purpose.
Yet there are ample reasons why we should not become complacent or take these
matters lightly.
Powers to screen and select for one purpose are immediately
available to screen and select for another purpose; the same is true for powers
of directed genetic change. And, as already noted, it is sometimes hard to
distinguish between desirable traits that one would call “healthy” and those
that one would call “good in some other way”: consider the case of leanness
(non-obesity) or perfect pitch (non-tone-deafness) or attentiveness
(non-distractibility). Moreover, there is ample reason to take stock of the
ethical and social issues related to present and anticipated practices of
screening and selection even if, as we have indicated, there is no reason for
alarm regarding “designer babies.” For the confluence of ever more
sophisticated techniques of assisted reproduction with ever greater capacities
for genetic screening and manipulation is already increasing the intrusion of
science and technology into human procreation, yielding to scientists and
parents ever growing powers over the beginnings of human life and the native
capacities of the next generation. In addition to welcome consequences for the
health of children, such practices may have more ambiguous or worrisome
consequences for our ideas about the relation of sex and procreation, parents
and children, the requirements of responsible parenthood, and beliefs in the
equal worth of all human beings regardless of genetic (or other) disability.
Before one can decide whether these changes should be
welcomed enthusiastically, tolerated within limits, or met with disquiet, one
must try to think through what they mean—for individuals, for families, and for
the larger society. In what follows, we shall examine, first, the reasons why
many people welcome these technologies; second, concerns that might be raised
about the safety of these procedures and about equality of access to their use;
and, finally, more profound ethical questions regarding how these technologies
might affect family life and society as a whole.
1. Benefits.
There is no question but that assisted reproductive
technologies have, over the past few decades, enabled many infertile couples to
conceive and bear children, and that the more recent addition of PGD holds the
promise of helping couples conceive healthy children when there is a serious
risk of heritable disease. The widespread practice of prenatal screening in
high-risk pregnancies has enabled numerous couples to terminate pregnancies
when severe genetic disorders have been detected. It is the natural aspiration
of couples not only to have children, but to have healthy children, and these
procedures have in many cases lent crucial assistance to that aspiration.
People welcome these technologies for multiple reasons: compassion for the suffering
of those afflicted with genetic diseases; the wish to spare families the
tragedy and burden of caring for children with deadly and devastating
illnesses; sympathy for those couples who might otherwise forego having
children, for fear of passing on heritable disorders; an interest in reducing
the economic and social costs of caring for the incurable; and hopes for
progress in the overall health and fitness of human society.xi
No one would wish to be afflicted, or to have one’s child afflicted, by
a debilitating genetic disorder, and the new technologies hold out the prospect
of eliminating or reducing the prevalence of some of the worst conditions.xii
Should it become feasible, many people would have reason to
welcome the use of these technologies to select or produce children with
improved natural endowments, above and beyond being free of disease. Parents,
after all, hope not only for healthy children, but for children best endowed to
live fulfilling lives. At some point, if some of the technical challenges are
overcome, PGD is likely to present itself as an attractive way to enhance our
children’s potential in a variety of ways. Assuming that it became possible to
select embryos containing genes that conferred certain generic benefits—for
example, greater resistance to fatigue, or lowered distractibility, or better
memory, or increased longevity—many parents would be eager to secure these
advantages for their children. And they would likely regard it as an extension
of their reproductive freedom to be able to do so; they might even regard it as
their parental obligation. In a word, parents would enjoy enlarged freedom of
choice, greater mastery of fortune, and satisfaction of their desires to have “better
children.” And, if all went well, both parents and children would enjoy the
benefits of the enhancements.
2. Questions of Safety.
Needless to say, the matter is hardly this simple. As with
all biomedical interventions, a primary ethical concern is the matter of
safety: the risks of bodily harm incurred by those subject to the procedures
involved in genetic screening and manipulation. As with all biomedical
interventions in reproductive processes, the safety issue takes on special
gravity and difficulty, precisely because some of the hazards will be inflicted
on the unconsenting child-to-be, and in the very activities connected with his
coming-into-being. The Council has previously dealt at length with this issue
in its report on human cloning, Human Cloning and Human Dignity, to
which the reader is referred.11
There are, first of all, hazards connected to the various
technological means employed in genetic screening and manipulation:
risks to the pregnant woman, the egg donor (if different from the
mother-to-be), and, most important, to the offspring. In the case of prenatal
screening, whether by amniocentesis or chorionic villus sampling, there are
well known, albeit slight, risks of infection, trauma (to both pregnant woman
and fetus), miscarriage, and premature labor. These risks are weighed against
the hazards of not screening, when the mother is of advanced reproductive age
or when there is other evidence suggesting heightened risk of genetic defects
in the fetus. Of course, prenatal screening serves to prevent genetic defects
only if it is followed up by abortion, which, besides destroying the fetus,
involves some potential health risks to the woman.
Regarding direct genetic manipulation of the germ line,
we have already examined some of the considerable associated risks and
uncertainties in the course of arguing that this technology is unlikely to be
applied to humans any time soon.
Regarding the topic of greatest interest here,
preimplantation diagnosis and selection, there are questions as to the
long-term safety of blastomere biopsy. Although the technique of removing one
or two cells from the eight-cell embryo for chromosome or DNA analysis does not
appear to harm the embryo (at least in those cases in which it goes on to
become a child), there are as yet no studies looking at long-term consequences
for children born after blastomere biopsy. Such currently imponderable risks
might be thought to recede in importance when severe genetic diseases are in
prospect. However, if PGD were to be undertaken, not to screen out genetic
defects, but to improve native powers, there should be heightened scrutiny of
any possible dangers involved in the procedure.
To date, ethical thinking about the hazards of the
techniques of assisted reproduction has often been incomplete, partly as a
result of the perceived desirability of the end. IVF and PGD are undertaken
with the intention of producing healthy, fit children; put this way, the
enterprise would seem to be much like other medical practices and, as such,
amenable to the same ethical standards. But a medical procedure designed to produce
a healthy person has a different character from procedures aimed at
safeguarding or healing a patient who is already alive. Yet here our thinking
is ill-served owing to a noticeable lacuna in our approach to the ethics of
risky therapies and (especially) the ethics of research using human subjects.
Ordinarily, when new technologies are introduced into
medical practice or when medical research is undertaken with human subjects,
the safety of the patients or subjects is of paramount ethical concern.
However, in the case of IVF, with or without PGD, the children who are produced
as a result of these procedures are not considered subjects at risk, for the
simple reason that the embryos being handled, tested, and manipulated are not
regarded as human subjects. Thus, blastomere biopsy performed on a tiny
eight-cell embryo is not treated as an experiment on a human subject or
as diagnosis of a patient, even though the future health and well-being
of the child are very much at stake. Instead, the ethics of IVF and PGD are
generally dealt with as though the only patient involved were the mother.xiii
Whether or not one believes that the embryo here manipulated is a fully human
being worthy of moral and legal protection, it is certainly the essential (and
fragile) beginnings of the child who will be born and whose health and
well-being should therefore be of overriding concern.
A deeper safety question connected with the goal of genetic
screening is whether the normal ethical standard—”the best interests of the
patient”—can be said to apply if and when PGD is used to select a “better”
child. Even when PGD is used only to screen out genetic diseases—and all the
more when it is employed to select positive traits—the parents are in effect
choosing a particular genotype for their child. The question is, will this
unprecedented power in the hands of the parents necessarily be used for the good
of the child? Should parents be willing to gamble the safety of their children
for the chance to make them “better than well”? What risks to their health and
safety are worth taking in pursuit of improvement or perfection?
Ordinarily, in most matters regarding children, our society
accepts the principle that each set of parents has authority and responsibility
for the well-being of their own children. Yet there are circumstances that lead
the state to step in to protect a vulnerable child against abusive or negligent
parents. In such cases, the best of parental intentions do not exonerate. How
should our society view parental (and biotechnical) discretion to seek to
produce “better children” through procedures carrying unknown hazards to those
children?
These questions take on greater poignancy once we recognize
a novel but morally significant feature of embryo selection using PGD, absent
in prenatal diagnosis. In intrauterine genetic screening, there is one
fetus being tested, and the question at issue is a binary choice of “keep” or “destroy.”
In contrast, in preimplantation screening a whole array of embryos are
scrutinized and tested, and the choice is not the either-or “yes or no” but
rather the comparative choice of “best in the class.” For if one is going to
the trouble of doing IVF supplemented by preimplantation diagnosis, why not get
“the best”—the healthiest and, perhaps soon, the “better-than-healthiest”? But
in order to get the best, or even in order to get a non-diseased child, one
must conceptually “bundle” all the separate embryos and regard them as if they
were a single precursor. All will be subjected to testing so that the one who
is chosen will be disease-free or better. Yet to make sure that the child who
is to be born is the fittest, rather than his diseased or inferior brother or
sister, the anointed one must bear potential risks (imposed during the testing)
that he would not have borne in the absence of the parental desire for
quality control. For the sake of which benefits to the child can we
justify imposing on him what kinds and what degrees of risk?
Before leaving the subject of safety and the concern for
the health of children, we observe an ironic feature of the search for better
babies with the aid of genetic screening. What if, as a result of widespread
genetic screening of adults and improvement in diagnostic screening of embryos,
the practice of IVF with PGD came to be seen as superior to natural
procreation in offering a greater probability of obtaining a healthy child? If
the procedures became sufficiently routine and inexpensive (to the point, say,
where they are covered by ordinary health insurance), prospective parents
interested in healthier (or otherwise better) children might increasingly be
tempted to consider IVF with PGD. Furthermore, couples who would then elect PGD
in order to screen out genetic diseases might well be tempted to engage at the
same time in some positive trait selection. In that case, what began modestly
as a means to help the infertile bear children and continued as a way to screen
out the worst genetic defects might ultimately stand as a competitor to natural
reproduction altogether, with significant consequences for the family and for
society at large.xiv
As this discussion indicates, the issue of health and
safety proves, on further reflection, to concern more than safety. When
biomedical technology permits the substitution, for natural procreation and the
rule of chance, of a procedure in which parents begin to control their child’s
genotype, reproduction becomes to some extent like obtaining or making a
product to selected specifications. Even if the parents are guided by their own
sense of what would be a good or perfect baby, their selection may serve to
satisfy their own interests more than that of the child. The new technologies,
even when used only to screen out and get rid of the sick or “imperfect,” imply
a changed attitude of parents toward their children, a mixture of control and
tacit expectations of perfection, an attitude that might grow more pronounced
as the relevant techniques grow more sophisticated. Apparently good
intentions—to improve the next generation, to enhance the life of our descendants—will
not guarantee that genetic screening will be an unqualified blessing for
parents and children. (We return to this subject shortly.)
3. Questions of Equality.
Many observers have noted with concern that, owing to the
sheer expense of IVF and PGD—a successful assisted pregnancy costing, on
average, roughly $20,000-$30,00012 xv—not
all couples who could benefit from these procedures have unfettered access to
them. If PGD were to become an established option, but only for the affluent,
one envisages the troubling prospect of a society divided between the
economically and genetically rich, on the one hand, and the economically
and genetically poor on the other. Severe inherited diseases might
disappear except among the poor, while genetic enhancement through screening
and selection might be a privilege enjoyed exclusively by the rich. These
concerns would, of course, diminish (though they would not disappear) if, as
seems likely, the costs of the procedures in question come down and access to
these services grows wider.xvi
Yet these legitimate concerns about equality of access
rest, ironically, on certain inegalitarian assumptions that need to be
brought to light. First, the goal of eliminating embryos and fetuses with
genetic defects carries the unspoken implication that certain “inferior” kinds
of human beings—for example, those with Down syndrome—do not deserve to live.
The assumption that the genetically unfit ought to be prevented from being born
embodies and invites a profoundly denigrating and worrisome attitude toward
those who do get to be born. How will we come to regard the many people
alive today who carry genetic defects that in the future will be screened out,
or the many people, even in a future age of more widespread screening, who will
still be born with the abhorred disabilities and diseases? The worry over
unequal access to PGD is, in effect, a worry about the inability of the economically
poor to practice the ultimate discrimination against the genetically
poor.
Second, when new techniques permit parents to be the
partial authors of their child’s genetic makeup, the inequality between parents
and children is substantially increased. Parents thereby acquire the power, not
just of giving life to their children, but of shaping (or trying to shape) the
character of that life. Of course, through education and upbringing parents
have always had an enormous influence on the lives of their children; but
inasmuch as the consequences of genetic screening are imposed before birth and are
carried as the child’s permanent biological destiny, the inegalitarian effect
of the new technology is unprecedented and irreversible.
In response to these concerns, it will be pointed out,
rightly, that genes are not exactly destiny, and that it will prove very
difficult to intervene genetically at the embryonic stage in ways that will
guarantee the appearance of the desired “improvements” in one’s children.
But much mischief can be done to a child simply from the enhanced parental
expectations, all the more so if the child fails to attain the superior native
gifts for which he was selected. And as we shall soon see, we are already
witnessing certain subtle forms of genetic discrimination even though the
technology of screening is still very undeveloped.
4. Consequences for Families and Society.
Beyond questions of safety and equal access, there is
reason to believe that the advent of expanded genetic screening and its uses in
reproduction could have a profound impact on human procreation, family life,
and society as a whole. At present, fewer than 10,000 children have been born
following PGD, and the screening procedure itself is being used to diagnose
only a limited number of chromosomal and genetic ailments. For these reasons,
it is both difficult to predict and also easy to underestimate the societal
import of marrying genomic knowledge with established techniques of assisted
reproduction, should the practice become widespread.
To make vivid the possible implications, it may therefore
be helpful to imagine a future time at which all external barriers to the use
of these procedures have been largely removed.xvii
Suppose that, a decade from now, IVF and PGD have been perfected to the point
where preimplantation screening is safe and effective, not prohibitively
expensive, and capable of identifying a wide range of markers for heritable
disorders. Suppose, in other words, that prospective parents (perfectly fertile)
routinely have the option of using these technologies in order to select an
essentially disease-free embryo for transfer to the mother’s womb.xviii
Under such circumstances—admittedly quite
hypothetical—might not the practice become moderately widespread? Could many
people come to regard using IVF plus PGD as safer (for the child) than the
randomness of sex, and therefore preferable to natural procreation even when
there is no particular history of genetic disease? In societies in which people
are limited—or limit themselves—to only one child, might they not increasingly
turn to these techniques to ensure that their child might be as “perfect” as
possible? And, should this procedure begin to compete with or even to supplant
sex as the more common route to conceiving children, in what ways would the
meaning of childbearing be altered?
The hypothetical case just sketched may seem like science
fiction, but the important questions it raises are, in fact, implicated in the
current practice of genetic screening. Even though the practice of PGD is still
in its infancy, its availability has begun to influence our thinking about
childbearing. Already the goals of assisted reproductive technologies are
changing, from the original modest aim of providing children for the infertile
to the novel and more ambitious aim of producing healthy children for whoever
needs extra assistance in obtaining them.xix
Anticipating the coming of augmented powers of genetic screening and selection,
people are expanding the idea of “a healthy child” and therewith almost
certainly the aspirations of prospective parents. In his presentation to the
Council, Dr. Gerald Schatten, a leading researcher in the field of reproductive
biology, stated that the overall goal of assisted reproductive technology is “to
help prospective parents realize their own dreams of having a disease-free
legacy” (emphasis added).13
The dream of a disease-free legacy—as stated, a goal that looks beyond merely
the next generation—seems rather different from the merely hopeful wish for a
healthy child. And even without such a broad ambition, the intervention of
rigorous genetic screening into the order of childbearing will likely involve
raising the standard for what counts as an acceptable birth. The likely
significance of this fact is subtle but profound. The attitude of parents
toward their child may be quietly shifted from unconditional acceptance to
critical scrutiny: the very first act of parenting now becomes not the
unreserved welcoming of an arriving child, but the judging of his or her
fitness, while still an embryo, to become their child, all by the standards of
contemporary genetic screening. Moreover, as the screening technology itself
grows more refined, more able to pick out serious but not life-threatening
genetic conditions (from dwarfism and deafness to dyslexia and asthma) and then
genetic markers for desirable traits, the standards for what constitutes an
acceptable birth may grow more exacting.
With genetic screening, procreation begins to take on
certain aspects of the idea—if not the practice—of manufacture, the
making of a product to a specified standard. The parent—in partnership with the
IVF doctor or genetic counselor—becomes in some measure the master of the child’s
fate, in ways that are without precedent. This leads to the question of what it
might mean for a child to live with a chosen genotype: he may feel grateful to
his parents for having gone to such trouble to spare him the burden of various
genetic defects; but he might also have to deal with the sense that he is not
just a gift born of his parents’ love but also, in some degree, a product of
their will.
These questions of family dynamics could become even more
complicated when preimplantation genetic screening is used to select embryos
for some desirable traits. While current negative screening is guided by the
standard of a healthy or disease-free baby, the goals of prospective positive
use are in theory unlimited, governed only by the parents’ ideas of what they
want in their child. Today, parents using PGD take responsibility for selecting
for birth children who will not be chronically sick or severely disabled; in
the future, they might also bear responsibility for picking and choosing which “advantages”
their children shall enjoy. Such an enlarged degree of parental control over
the genetic endowments of their children cannot fail to alter the parent-child
relationship. Selecting against disease merely relieves the parents of the fear
of specific ailments afflicting their child; selecting for desired traits
inevitably plants specific hopes and expectations as to how their child might
excel. More than any child does now, the “better” child may bear the burden of
living up to the standards he was “designed” to meet. The oppressive weight of
his parents’ expectations—resting in this case on what they believe to be
undeniable biological facts—may impinge upon the child’s freedom to make his
own way in the world. Here we see one of the ethically paradoxical consequences
of the new screening technologies: designed to free us from the tyranny of our
genes, they may end up narrowing our freedoms as individuals even further.
In addition to changes in the parent-child relationship,
there are reasons to be concerned about the wider social effects of an
increased use of genetic screening and selection. There is, first of all, the
prospect of diminished tolerance for the “imperfect,” especially those born
with genetic disorders that could have been screened out. It is offensive to
think that children, suffering from “preventable” genetic diseases, should be
directly asked, “Why were you born?” (or their parents asked, “Why did you let
him live?”). Yet it is almost as troubling to contemplate that “defective”
children and their parents may be treated contemptuously and unfairly in light
of such prejudices, even if they go unspoken. Already, parents who have a child
with Down syndrome are sometimes asked, “Well, didn’t you have an amnio? How
did this happen?” Many of these parents are people who, for their own ethical
reasons, have chosen to proceed with the pregnancy even after learning the
results of genetic screening, electing to love and care for the children that
it has been given to them to love. Yet as the range of detectable disorders
increases, as adult screening becomes ubiquitous and every pregnancy is tested,
and as the economic cost of caring for the afflicted remains high, it may
become difficult for parents to resist the pressure, both social and economic,
of the “consensus” that children with sufficiently severe and detectable
disabilities must not be born.
In all likelihood parents will increasingly feel pressure
to conform to shifting social standards of what is genetically fit. Along with
the freedoms bequeathed by the new technologies comes a certain danger of
social coercion and tyranny of public opinion. Furthermore, as our table of
detectable genetic markers grows more complete, there is the prospect of using
genetic screening to weed out not only the most devastating genetic disorders
but also heritable conditions that are bad but manageable, or even merely
inconvenient. In practice, it is likely to prove very hard to draw a bright
line between identifiable defects that might justify discarding an embryo or
preventing a birth and those defects that parents might (or should) be able to
find acceptable. It is not clear what resources our society will be able to
draw upon to assist parents in making such important decisions.
Should PGD and IVF, contrary to current expectations, ever
become widely used for positive screening of desirable traits, the impact on
society could be even greater. Our knowledge of the human genome and our powers
of genetic selection might grow so great as to unleash competition among
parents eager to bear children who are biologically destined to be taller,
thinner, brighter, or better-looking than their peers.
It should be noted that the social consequences of the
widespread use of genetic screening alone are likely to outstrip the actual
biological enhancements: those “unfortunate” enough to be born with genetic “defects”
that might have been detected by screening might well be subject to
discrimination, even without waiting to see how they turn out. The thoughtful
(if not quite scientifically accurate) film Gattaca explores some of the
chilling social implications of a human future in which genetic screening of
children has become the norm. To the careful observer of current practices, the
risks of such discriminatory implications are already evident.
II. Choosing
Sex Of Children
There is one area in which parents are today already able
to choose an important inborn characteristic of their children: sex selection
and control. This practice is widespread in many countries around the world,
and there is some evidence that it is being used with growing frequency in the
United States.14
Strictly speaking, choosing the sex of children is not exactly a choice for a “better”
child, save in those cultures in which one sex (usually male) is held to be
superior or privileged (or more rewarding to the family economically). But, if “good”
means “that which is desired,” it is a choice for a child thought by the
parents to be “better” in the limited, but significant, sense of “more wanted.”
In choosing a child of the preferred sex, the parents are acting to satisfy
their own desire for what, to them, is better (at least here and now).
While it is true that what is being chosen here is
nothing new or different—selection is confined to one or the other of the
eternal alternatives, male or female—the choice is not for that reason trivial
or free from moral implications. Parents choose a supremely important aspect of
their child’s lifelong identity, yet in most cases they do so not for the child’s
sake. They choose not because they think that the child will be better off
being male rather than female, or the reverse, but because they now want a boy
or a girl, or because they want to balance a family now lacking in one sex or
the other.xx
The seemingly innocent practice of sex selection in fact
raises many of the larger ethical concerns introduced above: about changing the
relations between parents and children, moving procreation toward manufacture,
and expanding parental choice and mastery over the next generation. Moreover,
what happens in the area of sex-selection may have implications for other, more
far-reaching efforts to choose or control the genetic makeup of our offspring,
if and when that becomes possible. Both for itself and as a precedent, it is
worth considering on its own this more modest form of seeking “better children.”
In considering the ethical implications of sex selection,
we must attend especially to the social consequences not just of the fact
of choice but of the choices made. For the private choices made by
individuals, once aggregated, could produce major changes in a society’s sex
ratio, with profound implications for the entire community—and also its
neighbors. Over the past several decades, disturbing evidence has accumulated
of the widespread use of various medical technologies to choose the sex of one’s
child, with a strong preference for the male sex. The natural sex ratio at
birth is 105 baby boys born for every 100 baby girls. But in several countries
today the ratio approaches or even exceeds 120 baby boys born for every 100
girls. There is also evidence that the ratio at birth of boys to girls is
rising among certain ethnic groups in the United States. This phenomenon
especially calls out for our attention and demands a broad-ranging ethical and
social evaluation.xxi
A.
Ends and Means
Sex selection offers a stark example of the marriage that
can occur between modern technique, on the one hand, and ancient custom or
primordial desire, on the other. For the human desire to choose the sex of one’s
offspring—usually to have a son rather than a daughter, but also on occasion a
daughter rather than a son—is hardly new. The folk wisdom of times gone by
attests to the enduring power of this human want, found in mothers and fathers
alike. In ancient Greece, it was believed that if men had sex while on their
right side, a boy would result; and in eighteenth-century France, it was
recommended to men who wanted sons to tie off their left testicle during
intercourse. In our own time, books that claim to reveal the secrets of having
a boy or a girl abound, with one bestseller recounting myriad methods but
recommending the timing of sexual intercourse as the key. Indeed, the
importance to all of us of a baby’s sex is revealed in the first question we
nearly always ask upon news of a newborn (assuming that we have not already
found out by sonogram): “Is it a boy or a girl?”
If the central importance of a baby’s sex and our desires
to choose it are old, the medical techniques for realizing our desires are new.
The principal means for doing so are, first, prenatal diagnosis (either using a
sonogram to disclose the genitalia or using amniocentesis or chorionic villus
sampling to disclose whether the karyotype is XX, female, or XY, male), followed
by abortion of fetuses having the unwanted sex. Second, preimplantation genetic
diagnosis (PGD) followed by selective transfer of embryos having the desired
sex. And third, a less certain technique, pre-fertilization separation of sperm
into X- and Y-bearing spermatozoa,xxii
followed by artificial insemination or in vitro fertilization. The first two
techniques select post-conception; the last seeks to produce the desired sex at
the time of conception.
These methods were developed (or at least the first two
were) to prevent disease. However, as with many other medical technologies,
nontherapeutic uses were quickly discovered and put into practice. The
techniques of amniocentesis and sonograms have been available respectively
since the 1970s and 1980s and have become increasingly widespread.
Amniocentesis can make a determination of sex at 16 to 18 weeks of gestation;
sonograms at 15 to 16 weeks. PGD, the procedure (described earlier) to screen
IVF embryos for chromosomal abnormalities and genetic diseases, has been
available for about ten years. The newer and less tested sperm-sorting
technology was originally a creation of the U.S. government, invented by a Department
of Agriculture scientist in the 1980s for the purposes of selecting sex in
livestock. The Genetics and IVF Institute in Fairfax, Virginia, developed the
technology for humans and currently has an exclusive license on it—the
technology is known as “MicroSort.” The Institute charges about $2,300 per try,
and currently claims a 90 percent success rate for girls and 73 percent success
rate for boys. It offers this service only for the purpose of “family balancing”—that
is, for achieving a mix of boys and girls in a family.
Even in just the short time that these various methods of
sex selection have been available, they have had dramatic effects on sex ratios
in many parts of the world. Generally, any variation in the sex ratio exceeding
106 boys born per 100 girls born can be assumed to be evidence of the practice
of sex selection. Here, from the most recent figures available, are just a few
examples of skewed sex ratios around the world today. The sex ratio at birth of
boys to 100 girls in Venezuela is 107.5; in Yugoslavia 108.6; in Egypt 108.7;
in Hong Kong 109.7; in South Korea 110; in Pakistan 110.9; in Delhi, India,
117; in China 117; in Cuba 118; and in the Caucasus nations of Azerbaijan,
Armenia, and Georgia, the sex ratio has reached as high as 120.xxiii
While the sex ratio in the United States has remained stable at 104.8, certain
American ethnic groups have seen a statistically significant rise in their sex
ratios. In 1984 the sex ratio for Chinese-Americans was 104.6 and for Japanese
Americans 102.6; in 2000, these ratios had risen respectively to 107.7 and
106.4.15
Imbalances in the sex ratio are certainly not evenly spread
across every region of the globe. However, one cannot but be impressed by the
fact that distortions in the sex ratio afflict developed as well as
underdeveloped nations, Hindu and Moslem populations as well as Christian
populations, Western as well as non-Western nations, wealthy and educated
regions as well as those that are less so. Although the practice is, for now,
greater outside than within the United States, the other nations are mainly
using technologies that we have developed (albeit for other purposes). One can
only expect in the future that technologies of sex selection will be further
refined and that new and cheaper technologies will emerge on the market. In the
absence of some system of regulation, nothing stands in the way of a
continuation and expansion of substantial distortions in the sex ratio, at
least in some parts of the world and among some communities in the United
States.xxiv
B. Preliminary Ethical Analysis
Previous public discussions of the ethics of sex selection,
conducted largely in terms of “sex bias” and “reproductive freedom,” have been
oddly ambivalent. On the one hand, despite the widespread and growing practice
of sex selection, it has attracted few overt defenders or partisans, at least
in the United States. Almost no one argues openly in its favor, and those who
do rarely offer up the single most important reason for its spread—the desire
for sons over daughters (though, as we shall see, this taboo may be changing).
To date, several special panels and advisory bodies in the United States have
considered the ethics of sex selection.16
None of these has condoned the practice; all have raised serious ethical
concerns. Yet, on the other hand, all have insisted that sex selection should
not be made illegal and may at least in some instances be defensible. Even
those who condemn the practice urge that there is nothing we can do about it
without violating our most cherished principles of reproductive freedom and
individual autonomy.
Typifying this approach, the one previous presidential
commission to consider the topic gave several reasons to support its judgment
that the use of amniocentesis and abortion for sex selection was “morally
suspect.” First, such a practice was “an expression of sex prejudice.” Second,
it was incompatible with the findings of developmental psychology that the
parent-child relationship depends upon “the attitude of virtually unconditional
acceptance.” Third, sex selection treated the child “as an artifact and the
reproductive process as a chance to design and produce human beings according
to parental standards of excellence”—an attitude that the commission condemned.17
Yet despite these powerful objections, the commission did not see the matter in
black-and-white terms either, and its policy recommendations were mild:
This is not to say that every decision to undergo
amniocentesis solely for purposes of sex selection is subject to moral
criticism. Nonetheless, widespread use of amniocentesis for sex selection would
be a matter of serious moral concern. Therefore, the Commission concludes that
although individual physicians are free to follow the dictates of conscience,
public policy should discourage the use of amniocentesis for sex selection. The
Commission recognizes, however, that a legal prohibition would probably be
ineffective and, worse, offensive to important social values (because vigorous
enforcement of any such statute might depend on coercive state inquiries into
private motivations).18
One factor distorting the ethical discussions of sex
selection in America is that it has become entangled—as has the debate over
stem cells and human cloning—in the controversy over abortion. Certain widely
accepted political and ethical principles, such as individual autonomy,
equality, the right to choose, and “non-directiveness,” are thought to be
threatened by any thoroughgoing critique of sex selection. In the early years,
when post-conception determination of sex followed by abortion was the only
means of sex selection, it was widely argued by many feminist-oriented
scholars, as well as other liberal thinkers, that any legal or policy actions
taken against abortion for sex selection would put the abortion right itself at
risk.
The practice of sex selection also throws other cherished
principles into disarray. Since the end of World War II, genetic counselors
have adhered to the ethical norm of “nondirectiveness.” It was hoped that by
this principle they would avoid the coercive eugenic policies of the past, from
forced sterilization to genocide. Yet by mandating the moral neutrality of
genetic counselors, nondirectiveness in fact makes it easier for individual
couples to practice sex selection as a matter of personal choice. And here too
the culture wars over abortion play a part. In one study it was found that
genetic counselors were reluctant to recommend against sex selection since they
considered it a “logical extension of parents’ rights to control the number,
timing, spacing, and quality of their offspring.”19
But three new developments conspire to invite a serious
reexamination of this matter. First, there is the growing cultural
heterogeneity of American society, with a rise in subgroups with distinct
preferences for males. Second, there are growing commercial prospects for these
services. Although the sex-selection technologies were originally developed
within the moral framework of medicine and were directed towards disease
prevention, the commercial possibilities of these technologies are becoming
increasingly evident. Sex-selection services are openly advertised on the
Internet, and sex selection could in the future become a big business.xxv
Third, perhaps related to the second, resistance to this practice is weakening,
including among those who are keepers and purveyors of the technologies.
In 1999, the American Society for Reproductive Medicine
(ASRM) criticized the use of PGD and sperm sorting for sex selection, fearing
that such practices might contribute to gender stereotyping and discrimination.20
In 2001, however, the ASRM relaxed its opposition to sperm sorting if used for
the purpose of “family balancing,”21
and, later that year, the chairman of ASRM’s ethics committee appeared to
endorse the use of PGD for the same purpose. When this produced considerable
public controversy, in part based on concern over the destruction of embryos
involved in PGD, the ASRM reaffirmed its position that PGD for sex selection
should be discouraged, in deference to concerns about gender bias as well as
about the moral status of the embryo. But the Society’s recommendations are not
enforced, and several of its members are openly offering sex selection to their
clients.
In sum, although the practice of sex selection continues to
grow, the American public debate over sex selection has never been aired in
full. The new impetus to the growth of this practice, from multiculturalism to
commercial interests, will make it difficult to slow its future spread. All the
more reason to try now to evaluate its significance, beginning with the most
common arguments for and against the practice.
* * *
There are a number of reasons given to support the practice
of sex selection. The most common rationale today for sex selection is that it
permits family balancing, enabling a couple to achieve its as-yet-unfulfilled wish
to raise both sons and daughters. Many parents have had three or four girls (or
boys) in a row, and really want a boy (or girl); effective sex selection would
satisfy this wish without any risk of continued “failure.” More generally, sex
selection is defended on grounds that it could increase the happiness of the
parents by enabling them to fulfill their desire for one or more sons or
daughters. Sex selection is also supported because it may help to slow
population growth (since many families continue to have children only to
achieve a particular balance of boys and girls); because it may enable parents
to fulfill religious or cultural expectations (since some cultures attach great
importance to or impose special obligations on male heirs); and because it may
make children feel more wanted and comfortable with their sex (since they will
know that they were in fact chosen to be whichever sex they are).
In certain cultures, the desire of parents for sons is
extremely powerful; in traditional Islam, for example, parents are expected to
continue bearing children until they have at least one son. A strong preference
for sons also appears prevalent in most (though not all) of the countries of
Asia. Sex selection can therefore be defended on “multicultural grounds,” as
helping parents to achieve not merely individual preferences but also
traditional and religious aims.
A common objection voiced against sex selection is that, in
its most prevalent practice today, it almost always involves the abortion of
(otherwise healthy) fetuses of the unwanted sex.xxvi
However, sex selection by IVF with PGD involves instead the selective transfer
of embryos of the desired sex and the discarding of any embryos of the other
sex; some people, for this reason, regard this approach as less morally
objectionable than the one that requires abortion, while others see no moral
difference. No such stigma attaches to the practice, still nascent, of sex
selection by sperm sorting; whether used with artificial insemination or in
conjunction with IVF, sperm sorting reduces the need to discard embryos of the
unwanted sex. Should ongoing research eventually produce selective spermicides
that would permit sex selection via natural intercourse, all such objections to
the means would be much diminished or even disappear. We would be left to
evaluate only the end itself.
The objection most often raised to sex selection,
especially as it is practiced throughout the world today, is that it reflects
and contributes to bias or discrimination against women. Sex selection has
involved the abortion of female fetuses on a massive scale, or, in a few cases
only, the selection of male embryos over female ones for implantation. As we
have seen, sex ratios in some communities have been altered sharply in a very
short period of time. Yet, criticism of this phenomenon has tended to be muted
because of the connection between sex selection and abortion; those who support
the right to an abortion have generally been reluctant to argue that abortion
for the sake of sex selection should be restricted. The “pro-choice” idea of “every
child a wanted child” establishes the rule in reproductive matters of the
supremacy of parental “wants.” Ironically, the “right to choose,” which was and
is defended in the name of equality for women, has in this way made permissible
the disproportionate choice of aborting female fetuses. It is open to question
whether the cause of equality has been well served by this development.
Paradoxically, the anti-female bias thought by critics to
be implicit in sex selection might in fact redound to the advantage of women,
at least regarding marriage: their relative scarcity could give them greater
selectivity, choice, and control of partners. In certain Asian countries for
example, where the ratio of boys to girls at birth has been severely skewed by
sex selection, young men of marriageable age are already facing a severe
shortage of young women to marry. Thus one might oppose sex selection as much
for the actual harm it does to men as for the prejudice it expresses against
women.
But sex selection is ethically troubling for reasons that
go beyond both its potentially discriminatory use and the necessity, under
current procedures, of destroying fetuses or embryos of the unwanted sex. One
of the fundamental issues has to do with the limits of liberty.
C. The Limits of Liberty
As we noted earlier, few policy makers or opinion leaders
argue openly in favor of sex selection. Rather, the assumption is made that our
most cherished ideals of individual autonomy and the right to choose preclude
an unambiguous condemnation of sex selection or public polices that might
curtail it. Yet this assumption is questionable.
Our society, to be sure, deeply cherishes liberty and
rightfully gives a wide berth to its exercise. But liberty is never without its
limits. In the case of actions that are purely self-regarding—that is, actions
that affect only ourselves—society tends to give the greatest protections to
personal freedom. But as we move outward, away from purely self-regarding
actions to those actions that affect others, our liberty is necessarily more
liable to societal and governmental oversight and restraint. Sex selection
clearly does not belong in the category of purely self-regarding action. The
parents’ actions (their choice of a boy or a girl) are directed not only toward
themselves but also toward the child-to-be.
One might argue that, since each child must be either a
girl or a boy, the parents’ actions in selecting the sex do not constitute much
of an intrusion on the prospective child’s freedom and well-being. But the
binary choice among highly natural and familiar types hardly makes the choice a
trivial one. And having one’s sex foreordained by another is different from
having it determined by the lottery of sexual union. There is thus at least a
prima facie case for suggesting that the power to foreordain or control the
nature of one’s child’s sexual identity is not encompassed in the protected
sphere of inviolable reproductive liberty. It is far from clear that either the
moral or the legal right to procreate includes the right to choose the sex—or
other traits—of one’s children.
But it is not only that sex selection affects the
individual child-to-be that puts it in a class of actions fit for oversight,
regulation, and (perhaps) curtailment. Sex selection, if practiced widely, can
also have powerful societal effects that reach far beyond individuals and their
families to the nation as a whole. The dramatic alteration in sex ratios in
such countries as South Korea and Cuba bear this out. Whether or not one views
the preference of individuals for sons over daughters as rational, taken
together these individual preferences could and do have serious society-wide
effects. The males may have diminished chances of finding an acceptable mate,
while the broader society may suffer from higher crime, greater social unrest,
increased incidence of prostitution, etc.—social troubles closely associated
with an abnormally high incidence of men, especially unmarried men.xxvii
One could argue that the choice of a male child is individually rational for
parents, given the strong preference in certain cultures for males. But such
individual choices may be socially costly—a case where individual parental
eugenic choices do not yield a social optimum. Indeed, unrestricted sex
selection offers a classic example of the Tragedy of the Commons, in which
advantages sought by individuals are nullified, or worse, owing to the social
costs of allowing them to everyone.22
In such cases, it is acceptable (and arguably necessary) for a liberal polity
to place limits on individual liberty.
D. The Meaning of Sexuality and Procreation
The two aspects of sex control—it is control of sex,
and it is a form of control of offspring—locate the deeper significance
of this practice in two important human contexts: the meaning of sexuality, and
the nature of procreation and family relations. A discussion of these matters
shows why there is more at stake here than personal liberty.
The arguments previously advanced against sex selection,
based on concerns regarding sexual bias, have been less than satisfactory. Some
have argued, for example, that sex selection would reinforce gender stereotypes
and threaten gender equality—presumably because it would manifest preferences
for boys. Yet these critics do not specify what they mean by “gender
stereotypes” and “gender equality.” Sometimes it seems that they are worried
that expressed preference for males would lead to a return to the world of
1950s-style stereotypes, with men and women playing distinct social roles. But
it sometimes seems that they are also worried that sex selection would threaten
a positive goal, a movement toward a more genuinely gender-neutral or socially
androgynous society, one in which our socially constructed human identities
would triumph over the mere biology of sexual difference. But in such a
gender-indifferent society, it would presumably make no difference whether you
are a girl or a boy, a woman or a man. And thus the choice of parents of a boy
rather than a girl, or vice versa, would have no negative implications of
gender stereotyping and would not threaten the equality of the sexes. The
choice between a girl and a boy would be purely an aesthetic choice—as between
pink and blue. And who could then object to letting parents choose? The very
logic and language of gender equality, taken in its androgynous direction,
would seem to soften opposition to sex selection. Further, there seems to be a
contradiction between arguing that “sex should not count” in opposing the right
of parents to choose boys rather than girls, while at the same time implying
that “sex counts plenty” in approving sex selection for “family balancing.” If,
as the critics say, sex does not or should not count, why could they think a
sexually balanced family humanly better than an unbalanced one? By selecting
sex for any reason, does one not in fact acknowledge that it is very
important?
As one of its arguments against the use of PGD for sex selection,
the ASRM has suggested that it might “trivialize human reproduction by making
it depend on the selection of nonessential features of offspring.”23
But if sexual identity is non-essential for many purposes (for example, at
least in theory, in employment or other areas where the law forbids
discrimination), for other purposes it is central to who and what we are.
Humanity exists as a sexually differentiated species; it is constituted in part
by the sexual difference. The reason is that our bodies are integral to our
humanity. There is no generic or androgynous human “self” to which, as a kind
of accidental addition, either a male or female body is then appended. Were
that the case, sexual identity really would be “nonessential” or “inessential”
to our self. It would not in any sense help to constitute a person’s identity.
If, however, we do not accept that kind of dualism in which
the real self simply is attached to and makes use of a (male or female) body,
then we will have to take sexual identity seriously as given with our body.
Every cell of the body and the entire body plan and form mark us as either male
or female, and it is hard to imagine any more fundamental or essential
characteristic of a person. It is surely odd, to say the least, to deny the
importance of sexual identity in the very activity of initiating a life.
Seeing this, we can understand why it often seems so
important to people that they have either a boy or a girl. Indeed, it would be
surprising if people did not care about a difference so fundamental. But
acknowledging this, we can also understand why we should be reluctant to see
ourselves as people who may appropriately dictate such a crucial part of the
identity of our child. Many prospective parents will say quite honestly that
they don’t care whether their baby is a boy or a girl; they’ll be happy to have
either. That attitude is desirable not because the sex of the child is a matter
of indifference but because it counts for so much. Far too much to be seen as
their responsibility to determine.
In a previous Council report, on human cloning,24
we emphasized how cloning-to-produce-children alters the very nature and
meaning of human procreation, implicitly turning it (at least in concept) into
a form of manufacture and opening the door to a new eugenics. Sex selection
raises related concerns.
The salient fact about human procreation in its natural
context is that children are not made
but begotten.
By this we mean that children are the issue of our love, not the product of our
wills. A man and a woman do not produce or choose a particular child, as they might buy a
particular brand of soap; rather, they stand in relation to their child as
recipients of a gift. Gifts and blessings we learn to accept as gratefully as
we can; products of our wills we try to shape in accordance with our wants and
desires. Procreation as traditionally understood invites acceptance, not
reshaping or engineering. It encourages us to see that we do not own our
children and that our children exist not simply for our fulfillment. Of course,
parents seek to shape and nurture their children in a variety of ways; but
being a parent also means being open to the unbidden and unelected in life.
Sex selection challenges this fundamental understanding of
procreation and parenthood. When we select for sex we are, consciously or not,
seeking to design our children according to our wants and desires. The choice
is never merely innocent or indifferent, since a host of powerful expectations
goes into the selection of a boy or a girl. In choosing one sex over the other,
we are necessarily making a statement about what we expect of that child—even
if it is nothing more than that the child should provide sexual balance in the
family. As fathers, we may want a son to go fishing with; or as mothers, we may
want a daughter to dress for the prom. The problem goes deeper than sexual
stereotyping, however. For it could also be the case that we may want a
daughter who will become president to show that women are the equal of men. But
in making this kind of selection we have hardly escaped the problem, for the
child’s sexual identity would be determined by us in order to fulfill some
particular desire of our own. If this were not the case then there would be no
felt need to choose the sex of our child in the first place. And thus does it
happen that in practicing sex selection our acceptance of our children becomes
conditional—a stance that is fundamentally incompatible with the deeper
meanings of procreation and parenthood.
The truth of this matter is paradoxically displayed by a
small fact connected with current American practices of sex-selection. The
assisted reproduction clinics that offer elective sex selection (through sperm
sorting or PGD) require their clients to agree in advance that they will accept
whatever child results, even if the child is not of the sought-for sex. The
clinics are no doubt mainly protecting themselves against legal liability for a
wrong result. Yet their need to insist on accepting an undesired “product”
shows how the practice itself must make into a matter of compulsory agreement
what the idea of parenthood should take for granted: that each child is ours to
love and care for, from the start, unconditionally, and regardless of any
special merit of theirs or special wishes of ours.
III. Improving
Children’s Behavior: Psychotropic Drugs
In addition to trying to enhance or control the inborn
capacities of their children, parents can try to improve what their children do
with the capacities they have. They can help them improve specific native gifts
(musical, artistic, athletic, etc.) through practice or training. They can
stimulate interest, develop tastes, and enlarge horizons through reading,
travel, and exposure to culture. They can try to improve their moods,
attitudes, and, of course, their behavior: how they act at home and school, how
they respond to authority, how they comport themselves with family and friends.
They can try to improve their ability and willingness to be considerate, show
respect, pay attention, carry out assignments, accept responsibility, deal with
stress and disappointment, and practice self-control. In these efforts, parents
continue to use, as they always have, our time-honored methods for child
rearing and education. But they may be acquiring extra help from biotechnology
and the novel approaches to behavior modification that make use of drugs and
devices that work directly on the brain.
Opportunities to modify behavior in children using
psychotropic drugs are growing rapidly, and the young but expanding field of
neuroscience promises vast increases in understanding the genetic and
neurochemical contributions to behavior and comparable increases in our ability
to alter it, safely and effectively. The variety of available drugs and the
range of conditions for which they are now or may soon be used is large and
growing. Today, stimulants (Ritalin, amphetamine, and the like) are the class
of behavior-modifying drugs most frequently prescribed to children, and they
are used almost exclusively for the treatment of
attention-deficit/hyperactivity disorder (ADHD). Selective serotonin reuptake
inhibitors (SSRIs)—such as Prozac and Zoloft—and other antidepressants, widely
prescribed for the treatment of mood and anxiety disorders in adults, are
increasingly being prescribed to children and adolescents for treatment of
depression, obsessive-compulsive disorder, tic disorders, and anxiety
disorders, including separation anxiety and school refusal. Neuroleptics, long
used to treat schizophrenia in adults, are now being used to treat children for
tics, schizophrenia and other psychoses, behavioral problems in autism, and
nonspecific aggression. Research is actively under way exploring the use of
mood stabilizers (for example, lithium) to treat children and adolescents for
bipolar disorder, oppositional defiant disorder, conduct disorder, episodic
explosiveness, and mood lability.25
A 2003 study found that the overall use of psychotropic drugs by children
tripled during the 1990s, in many cases approaching adult rates of utilization.xxviii
26
The growing availability of a wide range of
behavior-modifying drugs offers an ever-expanding armamentarium for parents
(and others) interested in trying to improve their children. Indeed, the mere
availability of such powerful new agents and knowledge of their effects will
invite many parents at least to consider their use, in order to realize more
effectively various aspirations they have for their children. And if other
people’s children are already using them for similar purposes, many parents may
feel pressed to give them a try, in order not to deny to their own child an
opportunity for greater success. Competitive behavior of many parents seeking
advantages for their children is already widespread in schooling and sports
programs; there is no reason to believe that it will stop at the border of
psychotropic drugs, should they prove effective and safe.
The wish of parents for “better children” most often takes
the form of a desire for children who are more well-adjusted, well-behaved,
sociable, attentive, high-performing, and academically adept. Parents are moved
not only by reasons of parental pride but also by the belief that children who
possess these qualities are more likely to succeed and flourish later in life.
These are perfectly fitting desires and proper motives, and we might well find
fault with parents who did not share them, at least to some considerable
degree. But the power to fulfill these aspirations through the dispensing of
drugs forces us to wonder both about the propriety of the means and also about
the desire for better children itself: how it should best be understood and
most responsibly be acted upon. What are the costs, including costs to good
conduct itself, of seeking improved conduct by this means? What are the costs,
including costs to flourishing childhood itself, of trying to secure our
children’s future success in life by overzealous efforts to guarantee their
achievements or govern their behavior?
Not surprisingly, the pursuit of better-behaved and more
competent children through the use of drugs, like the pursuit of better-endowed
children through the use of genetic technologies, has raised considerable
public disquiet and debate, both about means and about ends. The arguments have
been highly emotional, yet beneath the surface lie deep questions about the
meaning and responsibilities of parenthood. Because it involves children
already here (rather than children on their way to birth), this use of drugs
also confronts us with issues of moral education and character development, the
uniquely important yet limited freedom afforded to children, and the complex
meaning of childhood. It also challenges us to negotiate the often vague
boundary between what seems plainly to be therapeutic medicine and what seems
plainly to be parental or social control or performance enhancement. As with
behavior-modifying drugs used by adults, there is a potential conflict between
personal freedom and the need for prudence and restraint. But because the drugs
will often be given to young children incapable of making important decisions
for themselves, parents must also shoulder a complex and heavy burden of
responsibility—whether they choose to have their children medicated, or to
forego the advantages such medication might provide.
A. Behavior Modification in Children Using Stimulants
To consider these questions regarding behavior modification
in children, we have at our disposal a rich and illuminating case study. For
several decades now, stimulant drugs have been routinely used to alter the
behavior of children who are inattentive, impulsive, or hyperactive to an
abnormal degree. When the behavior in question is sufficiently severe, chronic,
and early in its onset, such children are held to suffer from
attention-deficit/hyperactivity disorder (ADHD). These children frequently
suffer greatly (as do their parents), especially as a result of failures in
school, disruptions at home, and the negative responses their behavior
generates from teachers, peers, and family members. Caring for them is often an
ordeal, affecting everyone in the vicinity. Fortunately, the symptoms
comprising ADHD respond well to prescription stimulants such as Ritalin
(methylphenidate) or Adderall (amphetamine). For the worst cases, these drugs
have proved a godsend, rescuing many a child from failure in school, trouble
with authorities, and general shame and opprobrium. In the great majority of
children diagnosed with ADHD, stimulant drugs (frequently used in combination
with non-medical efforts to alter behavior) have apparently succeeded in
enhancing focus and attention, calming disruptive behavior, and improving
performance at school. Moreover, their use by children also appears to be safe,
non-addictive, and free of major side effects. Thus, when prescribed for
children suffering from properly diagnosed and clear-cut cases of ADHD,
stimulants are not only an acceptable but a necessary treatment of choice, and,
until now, better than all other available alternatives.
Yet this good news comes with nagging concerns. In recent
years the rate at which children are diagnosed with ADHD and treated with
stimulants has risen dramatically. Although it is difficult to get precise
figures, it is estimated that up to four million American children are taking
Ritalin or related drugs on a daily basis.27
The rapid expansion of both ADHD diagnosis and Ritalin prescription has raised
troubling questions in some quarters. Because there is at present no definitive
biological marker for ADHD, its diagnosis—especially in borderline cases—can be
a matter of subjective judgment. This has aroused some concern about
misdiagnosis of ADHD and overprescription of Ritalin, especially in children
displaying less acute forms of distractibility and restlessness. The wide
variation in the incidence of stimulant prescription in different parts of the
United States has generated arguments about whether the drugs are
underprescribed (and ADHD underdiagnosed) in some communities or overprescribed
(and ADHD overdiagnosed) in others—or whether both may be true. Some observers
are also apprehensive because the drugs safely used in small doses in children
nonetheless belong to a family of powerful stimulants (amphetamines) that are
dangerous and addictive when snorted or otherwise abused by teenagers and
adults.
Our interest in this case study, however, is not driven by
concerns about the possible misdiagnosis of ADHD in children whose symptoms are
relatively mild or whose maladaptive behavior might have other sources. Rather,
we are interested in the use of psychotropic drugs to correct this
behavioral disorder because it provides an opportunity to consider what it
means in general to seek better or better-behaved children by
pharmacological means. For this purpose, several aspects of this case study are
especially relevant.
First, even when stimulant drugs are properly used to treat
a recognizable disorder, they are acting as agents of behavior modification and
control, applied by adults to children. It is aberrant behavior that justifies
their use; it is the diminution or elimination of said aberrant behavior that
is the measure of their success. Second, there are ambiguities in the set of
behaviors being treated: the symptoms clustered together under the diagnosis of
ADHD—inattentiveness and distractibility, hyperactivity, impulsiveness—can and
do exist separately and in varying degrees of severity, and they are always
targets of possible corrective intervention, regardless of diagnosis. Third,
these symptoms are continuous with unwanted behaviors found in children who do
not have the disorder; indeed, these behaviors are found to some extent in most
normal children at some time or another. Fourth, the very safety of these drugs
in children increases the temptation of parents to seek and physicians to
consider prescribing these agents as remedies for the undesirable behaviors.
Fifth, growing socio-economic pressures—from schools, clinics, advertising, and
health insurance reimbursement arrangements—are encouraging people to consider
such pharmacological approaches to controlling the behavior of children.
Finally—and perhaps most importantly—the stimulant drugs used to treat ADHD may
also be effective in correcting undesirable behavior and improving performance
even in the absence of a full-blown picture of ADHD. It is precisely their
effectiveness in improving attentiveness, focus, and steady conduct—coupled
with the absence of serious side effects when they are properly administered in
small doses—that makes these drugs attractive also for the treatment of
inattention, distractibility, and impulsivity in children who do not manifest
the full disorder. Indeed, these drugs have the capacity to enhance alertness
and concentration in children without any symptoms whatsoever.28
All these reasons conspire to make the use of stimulants to
control behavior a fascinating and important case study for the pursuit of “better
children” through psychopharmacology. None of us on the Council questions the
reality of attention-deficit/hyperactivity disorder. All of us believe that
children suffering its depredations should receive the best treatment
available, including prescription stimulants. Though we worry about misuse and
abuse, we are not opposed in principle to using behavior-modifying drugs in
children, even very young children, if circumstances require it. Though we
worry about the consequences of direct marketing of these drugs to parents, we
do not even begin with a decided prejudice against the use of drugs in
borderline cases, where the benefits to the child may outweigh the potential
harms and hazards. And we have no interest in passing judgment on the practice
of medicine in relation to ADHD or on the criteria for its diagnosis adopted by
the psychiatric profession.
Our purpose here is different. Taking our bearing from the
generalized capacities of these behavior-modifying drugs, we are mainly
interested in efforts to use them to achieve improvements in behavior and
performance that are independent of desires to heal disease. By considering the
implications of present and anticipated practices, we hope to shed light on the
promise and peril of a whole array of pharmacological avenues toward improving
our children. Given that anticipated advances in neuroscience will almost
certainly yield many new psychotropic drugs capable of altering various
behaviors, it is crucial that we prepare ourselves in advance to identify and
cope with the ethical and social implications of using them as agents of
control, enhancement, and behavior modification.
The story of stimulant use by children begins to paint a
picture of what it means to seek to modify children’s behavior through drugs,
both within but especially beyond the realm of therapy, and especially in the
light of the powerful social and cultural forces that are encouraging this
practice. By drawing some lessons from the story of stimulant use in children,
we shall try to add some depth and color to that picture and to suggest some
potential concerns that should be kept in mind as the technology advances and
its use increases. Should we succeed, this picture could function also as a
mirror in which we might be able to scrutinize all of our many efforts to
produce “better children.”
Before considering some ethical and social implications, we
pause to review some important aspects of the treatment and the behavior
treated.
1. What Are Stimulant Drugs?
The stimulants in question are, for the most part, two
related drugs: methylphenidate (sold under the brand name Ritalin, among
others) and amphetamine (sold under the brand name Adderall, among others). The
two are chemically similar (methylphenidate is in fact a synthetic derivative
of amphetamine), and their effects are analogous.xxix
They were not originally developed as
agents of behavior modification. They were first used in medicine in order to
raise and support blood pressure. Yet their stimulant effects on the central
nervous system have been known for many years, and these are today almost the
exclusive reason for their use. It is believed that they act primarily on the dopaminergic
neurotransmitter pathways of the brain, blocking reuptake at dopamine receptor
sites and therefore leading to increased dopamine concentrations between nerve
cells. Their effects seem especially focused on the pre-frontal cortex and the
locus ceruleus region of the brain, centers which are believed to be associated
with impulse control, inhibition, and cognitive functions related to choice and
action. Among their effects are diminished fatigue, improved concentration,
decreased distraction and restlessness, and enhanced effort on demand, as well
as increased blood pressure and greater physical strength, speed, and
endurance.
Such drugs can therefore have a powerful effect on behavior
and performance: concentrating the mind, calming the nerves, enhancing focus
and attentiveness. And indeed, behavior modification with the aid of
stimulants, including in children, is nothing new. Such drugs have been used by
physicians to temper hyperactive children since at least the 1930s,29
though such uses appear to have been extremely rare until the early 1960s. Over
time, the effectiveness of the drugs and the duration of their action have been
substantially increased, and their side effects have been decreased. Although
this class of stimulants can be prescribed for the treatment of narcolepsy, and
as an augmenter for certain antidepressants, they are by far most commonly
prescribed for the treatment of hyperactivity and disorders of attention. But
they are also used for their stimulant and performance-enhancing effects by
high school and college students, pilots and soldiers, and others eager to
enhance their alertness and attentiveness, say, for example, during test-taking
or combat.
Although they might be successful if tried, such drugs are,
of course, not just routinely used today to quiet any restless child. Because
of their addictive effects in adults, stimulants like Ritalin and Adderall are
not only prescription drugs; since 1971 they have been classified as Schedule
II controlled substances. This means their production is strictly monitored and
regulated by the federal Drug Enforcement Administration (DEA). Yet, closer to
the ground of action, their prescription and actual use by pediatricians and
other physicians are unregulated, and there is no scrutiny of off-label uses.
Moreover, because the drugs are so prevalent in most communities, owing to the
high incidence of ADHD, they can easily escape from professional control. It is
thus extremely difficult to prevent them from being shuttled around from
children being treated for ADHD to other users for other purposes.
2. Behaviors Inviting Improvement through Stimulant Drugs.
Compared with adults, many children, at many times, might
be described by those around them as restless, jumpy, impulsive, inattentive,
distractible, fidgety, overactive, and unruly. When persistent and severe,
these characteristics can be distressing to everyone in the vicinity, whether
at home, school, church, or playground. People begin to suspect that these
aberrant behaviors may be symptoms of some underlying disorder, neurological or
psychological. In order to help parents, teachers, and general pediatricians
sort out what degree and combinations of aberrant behaviors or symptoms deserve
medical or psychiatric intervention, behavioral and pharmacologic,
psychiatrists have set down diagnostic criteria for a family of attention
deficit and hyperactivity disorders.
The criteria for ADHD are set forth in the Diagnostic
and Statistical Manual of Mental Disorders, the standard American reference
for diagnosis of psychiatric disorders (now in its fourth edition, and often
called by a shorthand title, “DSM-IV”). They include serious symptoms of inattention,
impulsivity, or hyperactivity that persist for at least six months and that
cause significant impairment of function in more than one setting, whether
familial, social, academic, or occupational. The criteria further require that
at least some of the symptoms must have begun before the age of seven; as
defined, ADHD is thus a childhood disorder.xxx
(Readers are encouraged to examine the full text of the DSM-IV criteria,
presented in the appendix to this chapter.)
The causes of ADHD are not fully understood, yet the
current consensus appears to be that it is brought about by some combination of
genetic susceptibility and environmental factors.xxxi
Recent studies have shown that genetic factors contribute substantially, “with
most estimates of heritability exceeding 0.70,”30
and one study has located a major susceptibility locus for ADHD on a specific
portion of chromosome 16.31
Environmental risk factors seem to include traumatic brain injury, stroke,
severe early emotional deprivation, familial psychosocial adversity, and
maternal smoking during pregnancy. Yet despite the generic genetic and
environmental correlations, there is at present no clear biological marker or
physiological test for ADHD. The disorder is diagnosed solely on the basis of
observed and reported symptoms.
In florid cases, a symptom-based diagnosis is easy to make.
But the symptoms themselves shade over along a continuum into normal levels of
childish distractibility or impulsiveness, and, in all cases, evaluation is
unavoidably subjective. Degrees of attentiveness or self-command in children
distribute themselves normally, which is to say, around a bell-shaped curve.
And there is good reason to believe that the population of children who have
ADHD overlaps with children who appear in the low-end tail of the curve. As a
result, the purely symptomatic diagnosis of ADHD, even when made by experienced
experts after the requisite thoroughgoing examinations in home and school
settings, is always at risk of scooping up children who lack the disorder but
who are nonetheless comparably handicapped. Where the symptoms are less
clear-cut and less severe, diagnosis is fraught with difficulty.xxxii
Even the codified guidelines of DSM-IV reveal the difficulty: the Manual’s
classification of the types of ADHD lists, as an additional diagnostic
category, “ADHD, not otherwise specified,” a type of ADHD defined by “prominent
symptoms of inattention or hyperactivity-impulsivity that do not meet the
criteria for ADHD”32
(emphasis added).
This unavoidable vagueness in diagnosis tends to create
uncertainty with regard to appropriate treatment. In extreme cases, it is easy
to conclude that a child desperately needs a trial of treatment with
prescription stimulants. But in the cases of children who barely meet the
diagnostic criteria, or who barely fail to meet them, the challenge confronting
the child’s physician and parents is far more complicated, and the question of
whether to prescribe stimulants can be quite vexing.
Although estimates of how many children suffer from ADHD
vary widely, there seems to be little doubt that the numbers are rising.
Conservative estimates range between 3 and 7 percent of school-age children,
though only slightly more permissive criteria yield estimates as high as 17
percent.33
There is also disagreement concerning the cause of the increasing incidence of
the diagnosis. Have children always suffered this disorder in comparable
numbers, but without being either diagnosed or treated? Or is the increased
emergence of symptoms a reaction of today’s children to the peculiar stresses
of modern life, the changing expectations we have for our children, and the
tenuous character of many families and other institutions that should be
supporting them? How much of the increase is due to “diagnostic creep,” the
tendency of diagnoses to expand in accordance with the growing use of effective
behavior modification?
Although the DSM criteria are carefully set forth by
pediatric psychiatrists, many of the actual diagnoses are made by family
physicians lacking specialized training in these disorders, often on the basis
of brief visits and incomplete work-ups. Studies reveal widespread regional
differences in the frequency of diagnosis, as well as big differences among
various ethnic and racial groups. The true incidence of ADHD in children cannot
be determined from prescription stimulant use alone, since, for all of the
noted reasons, it is highly likely that Ritalin and similar drugs are both
over-prescribed and under-prescribed. Some children who receive the drugs
likely do not require them, while many children who are in need of treatment
are likely not receiving it.xxxiii
What is clear, however, is that stimulant prescriptions
have skyrocketed in recent years. The DEA attempts to calibrate its production
quotas to meet demand, so that production levels roughly correlate with
prescription levels. In the decade between 1990 and 2000, annual production of
methylphenidate increased by 730 percent, and annual production of amphetamine
increased by an even more astounding 2,500 percent.34
The overwhelming majority of those taking these medications are children,
though adult use has been growing rapidly. Estimates of the number of American
children taking Ritalin-like stimulants hover around three to four million.xxxiv
Recent reports also suggest that increasing numbers of very young children—as
young as two years old—are receiving prescription stimulants.35
These levels of prescription and use have created an entire
network of rules, procedures, and institutions within the American educational
system charged with identifying and accommodating those children who need or
use stimulant medications. In countless schools around the country,
distribution of the drugs to those students is a familiar daily routine, and a
generation of American students has grown up accustomed to the presence of
Ritalin and similar drugs in their schools and, if not in their own lives, in
the lives of their fellow students.
3. The “Universal Enhancer.”
The continuity of ADHD symptoms with ordinary behaviors,
the range of their severity, and the resultant difficulty of diagnosis is only
part of what opens the door to widespread use of stimulant drugs to control
behavior. The less-than-precise specificity of the behavioral problems is more
than matched by the non-specific enhancing effects of the drugs. As first
demonstrated by a groundbreaking NIH study in the 1970s, Ritalin has similar
effects on all children, regardless of whether they meet the criteria for ADHD.
Researchers found that normal boys (and normal adult men) and boys diagnosed
with ADHD had similar rates of improvement in performing certain mental tasks
when given Ritalin.xxxv
The stimulants brought the performance of the ADHD patients up to normal or
near-normal levels, and brought those of the normal subjects to above-normal
levels.36
Stimulants of this sort have therefore been called “universal
enhancers,” capable of modifying the behavior and improving the performance of
anyone who takes them. They will calm an unruly child, whether the child
suffers from a recognized psychiatric disorder or not, and they will enhance
the concentration and alertness of any user.
Herein lies the rub, and a chief source of our interest in
this subject in the present report. The fact that Ritalin and similar
stimulants can be, and quite possibly are being, used to mollify or improve
children who suffer no disorder except childhood and childishness suggests to
us another way in which biotechnology may affect future attitudes toward
rearing the young. Leaving aside all questions about the way in which ADHD is
understood and approached, we can learn a great deal from the public debates
concerning Ritalin use in children about the forces and pressures that
accompany the emergence and growth of the power to modify children’s behavior.
As the ability to modify and pacify behavior has increased, a network of
pressures, incentives, and attitudes in medicine, corporate America, the
educational system, the political system, and the general culture has formed
that tends to push in the direction of greater use of drugs—these and many
others. The deep desire for better children has for some found an outlet in
prescription stimulant use.
We have no doubt that, in most cases, parents, teachers,
and physicians are acting in what they sincerely deem the best interest of the
child. But anecdotes abound of schools and teachers pressuring parents to
medicate their children, often as a condition of continued enrollment; of
doctors, pushed by hectic schedules and distorted insurance rules, prescribing
stimulants to children they have not fully examined; and of parents seeking a
quick way to calm their unruly child or pressuring their doctors to give their
son the same medication that is helping his schoolmates.37
Powerful social pressures to compete, prominent in schools and felt by parents
and students alike, may play a role in encouraging extra stimulant use. The
Individuals with Disabilities Education Act, without intending to do so, has
created financial incentives for schools—and parallel incentives for parents—to
push for an ADHD diagnosis and treatment.xxxvi.xxxvii
Insurance requirements that tie reimbursement to diagnosis (rather than to
need) also conspire to push for more diagnosis and more drug treatment; so do
insurance rules that base doctors’ fee schedules on the number of visits with
patients and provide greater compensation for short visits offering drug
treatment than for longer sessions exploring behavior-changing approaches.
In a major (and worrisome) change from previous practice,
drug companies have taken to marketing drugs directly to parents, with spot ads
depicting miraculous transformations of anxious, lonely, or troublesome
children into cheerful, confident, honor-roll students. The presence in
virtually every community of children known to be gaining advantages from
stimulants creates a temptation for other parents to offer similar advantages
to their own children. In addition, strong evidence suggests the growing
illicit and self-medicating use of Ritalin and similar stimulants by high
school and college students, taken (often by snorting and at higher doses) to
enhance focus and concentration before important exams or while writing term
papers. Anecdotes do not make a trend or a rule, and we do not mean to suggest
that this is how Ritalin and similar drugs are usually used. But there is more
than ample cause for concern.
For it is clear that the potential for controlling and
modifying the behavior of children with such drugs already coincides with the
deeply felt desire for better-behaved, well-adjusted, sociable,
high-performing, happier children. This desire is felt not only by parents of
children who suffer from psychiatric disorders, but by every decent,
well-meaning parent of even the healthiest child. It is the desire to do what
is best for one’s child and to secure his or her present contentment and future
success. But when this desire is joined with the power to affect behavior
directly through biotechnology, its consequences may not serve the best
interests of children and parents. Indeed, the power to mold better children through
biotechnical interventions raises serious concerns.
B. Ethical and Social Concerns
Any use of behavior-modifying drugs by children calls for
special attention, not only because drugs might do damage to the body or brain
of the developing child, but also because the causes of human behavior, perhaps
especially in children, are always ambiguous and because a child’s behavior is
inherently transitory. If the targeted behavior occurred only in cases clearly
linked to an underlying medical abnormality, there would be no need for
discussion. But human conduct has so many intertwined roots—native biological
conditions, environmental factors, specific experiences, habits, beliefs,
moods, etc.—that it is rarely possible to pin down the exact source of a particular
“maladaptive” behavior. Even when an underlying disorder is unequivocally
present, it is hard to say with confidence that its presence alone made someone
act the way he did. Then, too, children are constantly changing as they grow,
and they complete the journey to adulthood by paths many and varied. In
children especially it can be difficult to distinguish between temporary
behavior problems that will resolve themselves later in life and long-term or
permanent aberrations that will respond only to medical treatment.
The crucial ethical and social issues therefore concern not
so much any possible harms to the brain or body produced directly or indirectly
by the medications—a problem shared with all drug use. What should concern us
most are the implications of inserting the novel and precedent-setting use of
drugs into child-rearing and educational practices, and what this means for the
character of childhood and the nature of responsible parenting. Yet responsible
analysis cannot omit a brief discussion of the safety of the drugs themselves.
For these are, as has been noted, dangerous and addicting chemicals.
1. Safety First.
No drug is entirely without risk of bodily harm, even when
used as directed. And common sense suggests that any drug whose brain effects
are powerful enough to alter behavior is powerful enough to do damage, perhaps
even as a result of its direct and immediate cerebral effects. Yet the
preponderance of the evidence shows a remarkably low incidence of side effects
when the stimulants are used, in low doses, in treatment of ADHD and allied
conditions. Unlike adolescents and adults who are often attracted by the
hepped-up feeling produced by amphetamines (appropriately named “Speed”), small
children do not like it. They are thus little tempted to move to the higher,
potentially addicting doses. While some have expressed the concern that
children who use stimulants when young might be more likely to become drug
abusers in their teens and beyond, there is evidence that the opposite is true.38
By avoiding the dismay and frustration of failure attached to untreated ADHD,
effective drug treatment early is thought to reduce the incidence of later drug
abuse (and other troubles with the law) in the afflicted population. Yet while
the benefits—both direct and indirect—of the treatment are well known, there is
not yet sufficient data regarding long-term and late-onset effects of having
been on stimulants for several years during childhood. We raise this matter not
to cast doubt on the reasonableness of drug treatment in clear-cut cases of
need where the benefits are great, but to raise a cautionary flag regarding any
behavior-improving uses that are purely “elective” and nontherapeutic.xxxviii
2. Rearing Children: The Human Context.
Rearing children is a uniquely complicated, difficult, and
important task. As we noted at the start of this chapter, parents must guide
and instruct their children while at the same time allowing them to develop to
their own potential and, to an extent, to follow their own path. The child has
his or her own wishes, wants, and inclinations, and a parent must discern which
of these are detrimental and should be corrected or countered, and which are
expressions of distinctive personality or identity that should be abided, met,
or encouraged. Parents know that their children must come to learn certain
difficult lessons, and that sometimes the learning is as important as the
lesson. But they also want to shield them from this world’s difficulties and to
make their path in life as free of burdens and dangers as possible. Parents
must navigate the narrow way between oppressive control of their children’s
lives and negligent deference to their children’s freedom. They know that
sometimes their own desire to do what is best for their child can run to
excess, and do harm inadvertently. This difficult balancing act often comes
down to allowing one’s good intentions to moderate one another.
The biotechnical capacity to modify children’s behavior
threatens to introduce an element into the mix that is so powerful as to be
very difficult to moderate. In an effective, safe, and relatively inexpensive
way, it would seemingly allow parents to help their otherwise healthy children
behave better, learn better, interact better, and perform better..xxxix
So why should any parent refrain from making use of behavior-modifying drugs?
In light of our above reflections, the following principal reasons or worries
present themselves: social control and conformity; moral education and medicalization;
and the meaning of performance.
3.
Social Control and Conformity.xl
Behavior-modifying agents would allow parents, teachers, or
others to intervene directly in a child’s neurochemistry when that child
behaves in a way that defies their standards of conduct. In some cases, the
children clearly benefit; in other cases, they do not. In all cases, the use of
such drugs to shape behavior raises serious questions concerning the liberty of
children.
The liberty of children is, of course, a complicated and
controversial concept. Children are not sufficiently mature, responsible, or
knowledgeable to make for themselves the most important decisions regarding
their lives. Choices about their health, their education, their activities,
their environment, and their future are made for them by others. And yet, we
all recognize certain limits to the degree to which they may be coerced or
restricted. If we take the trouble to think about it, we remember that children
are not just little adults and that their native gifts and dispositions come in
all shapes and sizes. Some are bold while others are cautious; some are
outgoing while others are shy; some are docile while others are seemingly
unteachable; some are independent and like their own company, others are
dependent and insist on sociability. We recognize that children, even very
young ones, display certain traits of personality and forces of will that ought
not simply to be repressed by others. Present and emerging
psychopharmaceuticals may increasingly enable us to affect and control these
traits in our children, and therefore to significantly restrict that liberty
that nature and society usually afford them. And whereas the overt behavior of
today’s overbearing parents may elicit a friendly reminder or a rebuke from
grandparents or neighbors—”Take it easy on him; he’s just a kid!”—the use of
drugs to attain similar goals proceeds out of sight, immune to the correcting eyes
of others.
Individual differences notwithstanding, childhood is
generally marked by a spirited rambunctiousness that, especially in the case of
young boys, often borders on sheer unruliness and hyperactivity. Curbing the
latter may too easily stifle the former, and with it an important part of
growing up. This would not only restrict the freedom of children, but alter the
very character of childhood. Because schooling is crucial (today perhaps more
so than before) to later success in a world that demands high cognitive skills,
we tend to forget that the temperaments selected over eons of evolution—perhaps
especially in males—are not obviously well-suited to sitting quietly in
classrooms or to the quiet demeanor that classrooms require. And because our society
insists that all children receive more or less the same kind of education (“No
child left behind”), we tend to ignore important individual differences and
instead tend to treat difficult or non-conforming children as problems. We fail
to consider that their spiritedness might be part of a more ambitious nature,
their lack of attention part of an artistic temperament, or their restlessness
a fitting response of genuinely eager students to uninteresting or poorly
taught classes.
A well-meaning teacher, confronted by an oversized class of
excitable second graders, might judge the most restless and disruptive among
them to be simply uncontrollable and potentially in need of treatment. The
busy, tired parents of an especially fidgety and energetic eight-year-old might
be tempted to seek pharmacological ways to help their child be more sociable
and attentive or do better in class. In some cases such children really will
need medical treatment to be able to perform even minimally. But in some cases
they won’t, and the increasing availability and popularity of the treatment may
diminish our ability to tell the two apart; or, more importantly, it may alter
our standards of when a child is in need of psychopharmaceutical intervention.
Using psychotropic drugs might become, for an increasing number of children, a
social necessity or expectation—merely to keep up.
This enhanced ability to make children conform to
conventional standards could also diminish our openness to the diversity of
human temperaments. As we will find with other biotechnologies with a potential
for use beyond therapy, behavior-modifying drugs offer us an unprecedented
power to enforce our standards of normality. Human societies have always had
such standards, but most societies (and certainly our own) have in practice
tolerated fairly significant deviations from them, and have greatly benefited
from such tolerance. Some proponents of the new biotechnologies suggest that
they will offer us new options and enlarge our capacity to exercise our individual
desires. Far from restricting variety, they contend that these new empowerments
would serve and increase the diversity of our society. The point is not without
merit. Yet diversity is not only a matter of options and choice, but also a
matter of innate inclination and temperament, strength of desire and
aspiration, and cultivated character. The power to stifle these latter traits
in the name of better behavior and elementary education seems likely to
diminish both the range of human types in our society and the range of the
choices we will finally make. This danger seems especially great with regard to
techniques of exercising control over children, since parents are more likely
to desire to help their children fit the mold and conform to the conventional
pattern than to seek social conformity for themselves. As the
physician-bioethicist Carl Elliott put it:
[T]he very changes that some people may think of as
unqualified “enhancements” (i.e., becoming more attentive and mindful) are not
quite as unqualified as they may initially think; . . . moreover, these
enhancements may well be changes critical to a person’s identity, a person’s
sense of who he or she is.39
In an age of routine and widely used agents of behavior
modification, the power to control our children would therefore raise
significant worries about the prospects for benevolently enforced conformity,
restriction of freedom, and perhaps even for the decline of genuine excellence.
4. Moral Education and Medicalization.
A further concern has to do with the substitution of the
language and methods of medicine for the language and methods of moral
education. Children suffering from ADHD and similar disorders genuinely lack
some degree of the capacity to impose their will on their behavior. If a child
has poor impulse-control equipment in his brain, repeated failure will not
produce self-command, but rather a loathing of it. Drugs could help get him to the
“level playing field,” after which time he might have a fighting chance to
enjoy a normal course of learning self-command. Yet most children whose
behavior is restless and unruly could (and eventually do) learn to behave
better, through instruction and example, and by maturing over time. Praise and
blame from parents and teachers, patient instruction and extra attention, as
well as the experience of performing poorly or well, can help strengthen the
will of the child, which slowly increases the child’s ability to control his or
her impulses and behavior.
Behavior-modifying agents circumvent that process, and act
directly on the brain to affect the child’s behavior without the intervening
learning process. If what matters is only the child’s outward behavior, then
this is simply a more effective and efficient means of achieving the desired
result. But because moral education is typically more about the shaping of the
agent’s character than about the outward act, the process of learning to behave
appropriately matters most of all. If the development of character depends on
effort to choose and act appropriately, often in the face of resisting desires
and impulses, then the more direct pharmacological approach bypasses a crucial
element. The beneficiaries of drug-induced good conduct may not really be
learning self-control; they may be learning to think it is not necessary. As
Dr. Steven Hyman put it in his presentation to this Council:
There are symbolic messages to children about
self-efficacy. Behavioral control comes from a bottle. We have the problem of
anabolic steroids for the soul.40
By slowly learning to master his or her impulses, a child
not only comes to behave well, but also learns to exercise genuine self-control
and some degree of self-mastery. The child grows more mature. By treating the
restlessness of youth as a medical, rather than a moral, challenge, those
resorting to behavior-modifying drugs might not only deprive that child of an
essential part of this education. They might also encourage him to change his
self-understanding, by coming to look upon himself as governed largely by
chemical impulses and not by moral decisions grounded in some sense of what is
right and appropriate.
This concern arises with a number of the biotechnologies we
will consider in this report. By medicalizing key elements of our life through
biotechnical interventions, we may weaken our sense of responsibility and
agency. And, technologies aside, merely regarding ourselves and our activities
in largely genetic or neurochemical terms may diminish our sense of ourselves
as moral actors faced with genuine choices and options in life. These concerns
are especially serious with regard to children, where those who are treated are
not the ones making the choice to seek treatment. Children learn by their
elders’ example, and in this instance they may learn from those whose opinions
matter most to them that behavior is simply a matter of chemistry, and that
responsibility for their actions falls not to themselves but to their pills.
They may behave better, but they will not have learned why, or even quite how.
5. The Meaning of Performance.
A distinct but closely related concern has to do with the
lesson taught to children about the significance of their abilities. Agents of
behavior modification, like Ritalin, Adderall, and future generations of such
drugs, are at the same time also agents of performance enhancement. We will
take up performance enhancement in its own terms in the next chapter, but our
interest here is in the modification of a child’s behavior by drugs given to
him by his elders.
Children’s behavior, in the limited context in which we
have been discussing it, is largely a matter of impulse control and
self-restraint. But performance is a matter of ability and skill, and
(sometimes) of one’s standing in competition with others. One’s assessment of
one’s own achievement and worth often has to do with how one performs in the
face of various physical and mental challenges. Building our abilities and
self-confidence—through study and practice over time—is an important part of
all of our lives, and an especially crucial element of childhood.
Parents understandably want their children to perform at
high levels, to stand with or above their peers, and to succeed. They know that
such things are crucial for any child’s future, and they want their child to do
as well as possible. But the introduction of performance-enhancing agents
confuses the picture, in this area as in the others. Artificial enhancement can
certainly improve a child’s abilities and performance (at least of specific
tasks, over the short run), but it does so in a way that separates at least
some element of that achievement from the effort of achieving. It may both
rob the child of the edifying features of that effort and teach the child, by
parental example, that high performance is to be achieved by artificial, even
medical, means. At the very least it sends a confusing message to the child
about the meaning of performance: one which at the same time puts too much
emphasis on the importance of performance, and too little emphasis on the
integrity of genuine ability and unaugmented merit.
The concerns with performance, together with the temptation
to seek to improve it through biotechnology, are felt first by parents, and in
a sense imposed on children by the parental decision to seek stimulants or
similar enhancers. But with time, as a child lives and matures knowing that
such agents of behavior modification and performance enhancement have been
integral to his life, the child himself may also come to feel the desire to
make use of such technologies. Performance enhancement will cease to be
imposed, and will come to be a choice, perhaps even more attractive than it is
today. In the remaining chapters, we will take up the subject of freely chosen
adult use of biotechnologies beyond therapy, and consider the sorts of desires,
ends, and means that may shape the human experience in the age of
biotechnology.
IV.
Conclusion: The Meaning Of Childhood
To this point we have indicated ways that the use of
biotechnical means can actually undermine the end of better children. But there
are also serious questions to be put to the goal itself, some about “childhood,”
some about what is “better.” Life is not just behaving, performing, achieving.
It is also about being, beholding, savoring. It is not only about preparing for
future success. It is also about enjoying present blessings. It is not only
about school, work, and networking. It is also about leisure, play, and
friendship. At no time of life are these truths more evident—and more
realizable—than in childhood. Life soon enough becomes serious, driven, and
hard. The sweetness, freshness, and spontaneity of life are available in their
purest form only to the as-yet-unburdened young.
Some observers of the present scene have commented ruefully
about the way in which much of modern life threatens the innocence and the
simple joys of childhood. People note with sadness how both a pragmatic concern
for their future successes as adults and a precocious introduction to the
troubles of the adult world are obtruding themselves into the lives of younger
and younger children. It would be paradoxical, not to say perverse, if the
desire to produce “better children,” armed with the best that biotechnology has
to offer, were to succeed in its goal by pulling down the curtain on the “childishness”
of childhood. And it would be paradoxical, not to say perverse, if the desire
to improve our children’s behavior or performance inculcated short-term and
shallow notions of success at the expense of those loftier goals and finer
sensibilities that might make their adult lives truly better.
Appendix
Diagnostic Criteria for Attention-Deficit/Hyperactivity Disorder
According to the American Psychiatric Association, to be
diagnosed with ADHD a patient must meet the following five criteria (A-E) (but
also see the category, “ADHD, not otherwise specified,” below):
A. Either 1 or 2:
1. Six (or more) of the following symptoms of inattention
have persisted for at least six months to a degree that is maladaptive and
inconsistent with developmental level:
Inattention
a. Often fails to give close attention to details or makes
careless mistakes in schoolwork, work, or other activities
b. Often has difficulty sustaining attention in tasks or play activities
c. Often does not seem to listen when spoken to directly
d. Often does not follow through on instructions and fails to finish
schoolwork, chores, or duties in the workplace (not due to oppositional
behavior or failure to understand instructions)
e. Often has difficulty organizing tasks and activities
f. Often avoids, dislikes, or is reluctant to engage in tasks that require
sustained mental effort (such as schoolwork or homework)
g. Often loses things necessary for tasks or activities (e.g., toys, school
assignments, pencils, books, or tools)
h. Is often easily distracted by extraneous stimuli
i. Is often forgetful in daily activities
2. Six (or more) of the following symptoms of
hyperactivity-impulsivity have persisted for at least six months to a degree
that is maladaptive and inconsistent with developmental level:
Hyperactivity
a. Often fidgets with hands or feet or squirms in seat
b. Often leaves seat in classroom or in other situations in which remaining
seated is expected
c. Often runs about or climbs excessively in situations in which it is
inappropriate (in adolescents or adults, may be limited to subjective feelings
of restlessness)
d. Often has difficulty playing or engaging in leisure activities quietly
e. Is often “on the go” or often acts as if “driven by a motor”
f. Often talks excessively
Impulsivity
g. Often blurts out answers before questions have been
completed
h. Often has difficulty awaiting turn
i. Often interrupts or intrudes on others (e.g., butts into conversations or
games)
B. Some hyperactive, impulsive, or inattentive symptoms
that caused impairment were present before age seven years.
C. Some impairment from the symptoms is present in two or
more settings (e.g., at school [or work] and at home).
D. There must be clear evidence of clinically significant
impairment in social, academic, or occupational functioning.
E. The symptoms do not occur exclusively during the course
of a Pervasive Developmental Disorder, Schizophrenia, or other Psychotic
Disorder and are not better accounted for by another mental disorder (e.g.,
Mood Disorder, Anxiety Disorder, Dissociative Disorder, or a Personality
Disorder).
Types of ADHD Using DSM-IV Criteria
ADHD,
predominantly inattentive type
If Criterion A1 is met but Criterion A2 is not met for the past six months.
ADHD,
predominantly hyperactive-impulsive type
If Criterion A2 is met but Criterion A1 is not met for the past six months.
ADHD,
combined type
If both Criteria A1 and A2 are met for the past six months.
ADHD,
not otherwise specified
This category is for disorders with prominent symptoms of inattention or
hyperactivity-impulsivity that do not meet the criteria for
Attention-Deficit/Hyperactivity Disorder. Examples include:
1. Individuals whose symptoms and impairment meet the
criteria for Attention-Deficit/Hyperactivity Disorder but whose age at onset is
seven years or after;
2. Individuals with clinically significant impairment who
present with inattention and whose symptom pattern does not meet the full
criteria for the disorder but have a behavioral pattern marked by sluggishness,
daydreaming, and hyperactivity.
* * *
Source: American Psychiatric Association, Diagnostic and
Statistical Manual of Mental Disorders, Fourth Edition, Text Revision,
Washington, D.C.: American Psychiatric Association, 2000, pp. 92-93.
_________________
Footnotes
i. The Repository for Germinal Choice, a California sperm bank
accepting deposits only from Nobel Laureates or other comparably accomplished
donors, recently closed its doors, having done only minimal business in the
roughly twenty-five years of its existence.
ii. Although a form of “negative” genetic selection, prenatal
diagnosis can give reassurance to prospective parents that such traits are
absent.
iii. Of course, the desired trait for which an embryo is selected
may in fact be simply the presence of a normal gene, lacking the feared genetic
abnormality.
iv. Cloning-to-produce-children (if not all human cloning)
could be considered yet another form of genetic control of the next generation.
After all, the aim of cloning is to secure a new life with a predetermined and
preferred genome. Cloning gives genetic control not only of a single trait but
of a whole person; the ethical issues attending other forms of genetic control
are, if not identical, similarly troubling. Many of these issues are explored
in this Council’s report, Human Cloning and Human Dignity: An Ethical
Inquiry, Washington, D.C.: Government Printing Office, 2002.
v. There is one exception that we will consider later, on its
own: the use of prenatal diagnosis and abortion for choosing sex of offspring.
Such sex selection is widely practiced in some parts of the world and, on a
more modest scale, in the United States. Choosing sex of children need not
involve genetic testing: a sonogram can make the diagnosis.
vi. Growing recognition of the complexity of gene interactions,
the importance of epigenetic and other environmental influences on gene
expression, and the impact of stochastic events is producing a strong challenge
to strict genetic determinism. Straightforward genetic engineering of better
children may prove impossible, not only in practice but even in principle.
vii. The Recombinant DNA Advisory Committee (RAC) of the
National Institutes of Health (NIH), responsible for ethical review of all
NIH-funded research proposals that involve putting genes into human beings, is,
as a matter of policy, not reviewing any proposals that seek to modify gametes
or embryos. This decision produces an effective moratorium on all such research
(at least that supported by federal funding). The Food and Drug Administration
(FDA) has recently shut down the practice of ooplasm transfer into eggs
undergoing in vitro fertilization, regarding it as a practice of unapproved
germ-line genetic engineering because ooplasm contains mitochondrial DNA.
viii. Although scientists are able to identify thousands of human
genes and their variants, the fact that at present blastomere testing is done
on the minute quantity of DNA present in one or two cells limits the reach of
PGD in any given embryo to a handful of genetic variants. However, ongoing
research on techniques for whole genome amplification will likely permit PGD in
the future to test simultaneously for hundreds or even thousands of genetic
variants in the same embryo. Of course, because of the complex relationship
between genes and traits, the mere ability to screen for multiple genetic
variants in no way guarantees that numerous phenotypic traits will soon be
detectable.
vix. Color-blindness, a single-gene defect, can already be
screened for.
x. If, for example, a desired trait required the
concurrence of only seven specific genetic alleles and (to take the simplest
case) there were only two alternate variants of each gene, one would need (on
the average) 128 embryos (and even more eggs) to get the full complement (2 to
the seventh power). (This point is powerfully illustrated in figures VIII.a-c
in the recent report of the German National Ethics Council, Genetic
diagnosis before and during pregnancy: opinion, Berlin: Nationaler
Ethikrat, 2003, pp. 158-160.) Today, in the average IVF cycle, twelve to
fifteen eggs are obtained by superovulation, and roughly only half make it to
the stage where screening could occur. Of course, if the oocyte supply could be
increased, say by deriving oocytes from embryonic stem cells, this problem might
be soluble.
xi. Not all Members of this Council agree that it is obviously
and simply good to assist people in avoiding the need to care for children who
are not healthy. One Member comments: “It would be good to live in paradise,
but, given that we don’t, I am not sure that it is necessarily a good not to
have to care for children who are not healthy. I would have thought it ‘good’
to try to produce people who—in a world that is not paradise—are able and
willing to shoulder such burdens.”
xii. We know of at least one exception: the case of a deaf
couple using genetic screening to produce a deaf child.
xiii. In several of its efforts to exercise authority over
practices connected with assisted reproduction, such as
cloning-to-produce-children or ooplasm transfer, the Food and Drug
Administration has had to resort to the fiction that the embryo is a “drug,”
whose “administration” to the mother is potentially hazardous—to her.
xiv. As early as 1971, only two years after the first
successful in vitro fertilization of human egg by human sperm (and well before
the birth of Louise Brown in 1978), geneticist Bentley Glass, in his
presidential address to the American Association for the Advancement of
Science, was heralding the eugenic possibilities of IVF. He looked to IVF,
coupled with genetic screening of gametes and embryos, not for the relief of
infertility but for securing “the right of every child to be born with a sound
physical and mental constitution, based on a sound genotype.” Glass went on to
predict: “No parents will in that future time have a right to burden society
with a malformed or a mentally incompetent child.” (Glass, B., “Science:
Endless Horizons or Golden Age,” Science 171: 23-29, 1971, p. 28.)
xv. A single reproductive cycle of IVF costs about $8,000, with
roughly a 30 percent chance of producing a baby; PGD adds $3,000 or more to the
cost of an IVF cycle and slightly reduces the chance of producing a baby.
xvi. Indeed, one could argue that, under such
circumstances, there may be greater relative gains for the poor than for the
rich, since the former can, to some degree, “catch up genetically.” Even if
genetic inequality persisted, the genetically poor might be better off than
they are now.
xvii. The discussion that follows is frankly speculative,
and only time may tell how accurate it is. Yet because the stakes are
potentially very high, this thought experiment is useful in clarifying what
such innovation could mean for human procreation and our attitudes toward
children.
xviii. The desire for a “disease-free” inheritance will be,
of course, difficult if not impossible to realize. All of us carry genetic
variants that predispose to illness; perhaps a few dozen for each of us. It is
highly unlikely that all of these can ever be screened out.
xix. A significant and growing fraction of Americans now
using assisted reproductive technologies are not infertile or seeking treatment
for infertility. Dr. Gerald Schatten informed the Council that up to a third of
couples who undergo IVF with PGD choose to do so without a history of
infertility. (See Dr. Schatten’s presentation cited in endnote 3.) In Europe,
according to a 2001 survey by the European Society of Human Reproduction and
Embryology, as many as three-quarters of PGD procedures are performed on
couples without a prior history of infertility or subfertility. (“ESHRE PGD
Consortium: data collection III [May 2001],” Human Reproduction, 17[1]:
233-246, 2002. See especially Table II: Reasons for preimplantation genetic
diagnosis.) At present we know nothing about the children born as a result, or
how they fare in their families.
xx. Of course, some parents may believe that a balanced
family, with both sons and daughters, is better not only for them but for all
their children. Alternatively, they might believe that boys need brothers and
girls need sisters, or that they (as parents) are better suited to raising a
child of one sex rather than the other. And, in societies with a deep cultural
belief in the superiority of males, parents might well think they are doing
their child a favor by selecting for maleness.
xxi. Our focus here is on the nonmedical use of sex selection—that is, sex
selection for purposes of choosing sex unrelated to the treatment or prevention
of disease. Sex selection can also be used to prevent the transmission of
sex-linked genetic diseases. For example, in the case of families carrying the
gene for hemophilia—an X-linked recessive disease, affecting only males—detection
and abortion of all male fetuses will prevent the birth of an afflicted child.
In such instances, a clear medical goal is being served. While some Members of
Council would question whether sex selection for this purpose is legitimate, or
even whether the prevention of disease by selecting for sex is the same as
treating a patient for disease, this discussion will not take up these more
general issues. Our goal is to examine sex selection for itself and to
understand what might be troubling about the practice apart from the issues of
elective abortion or the destruction of embryos. It is also worth noting that “sex
selection for medical reasons” is a misnomer. It is only incidentally a
selection for sex, but uses sex as the criterion for selecting against a
sex-based disease. Should genetic tests become available that would distinguish
the afflicted male fetus from the non-afflicted one, selection would no longer
be based on maleness, but solely on the presence or absence of the mutant gene.
xxii. For the time being, the separation is physical. But
researchers are also interested in finding immunological techniques that might
differentially find X- and Y-bearing sperm and destroy or deactivate the
undesired ones.
xxiii. Although data is lacking regarding the techniques
people in these countries use to produce these large shifts in the sex ratio,
we suspect that sonography-plus-abortion is by far the most common.
xxiv. If sex selection in the United States were practiced
largely for family balancing (the use of sex selection to help a couple with at
least one child to have another child of the less represented sex in the
family), it is unlikely that we would experience major distortions in the sex
ratio.
xxv. Here’s how Fortune magazine recently summed up
the potential market just for MicroSort alone: “Each year, some 3.9 million
babies are born in the U.S. In surveys, a consistent 25 percent to 35 percent
of parents and prospective parents say they would use sex selection if it were
available. If just 2 percent of the 25 percent were to use MicroSort, that’s
20,000 customers . . . [and] a $200-million-a-year business in the U.S. alone.”
(Wadman, M., “So You Want a Girl?” Fortune, 9 February, 2001.)
xxvi. Note that this is not an objection to the activity of sex selection
as such, but only to an aspect of the means used. Other objections, considered
below, address the thing itself: the choosing of sex, the choosing of sex,
and the social consequences of the choices made.
xxvii. At the same time, the preponderance of males may
encourage marriage, discourage cohabitation, and increase the proportion of
two-parent families, given that women, being scarce, could exert greater
control over the marriage market. See, for example, chapter 3 of the recent
book on marriage by Council Member James Q. Wilson (Wilson, J.Q., The
Marriage Problem: How Our Culture Has Weakened Families, New York:
HarperCollins, 2002). But a high incidence of marriage in sex-imbalanced
societies does not solve the social problem of the large number of unmarried
and unmarriable males.
xxvii. This study does not indicate the conditions for
which these drugs are being prescribed. The mere increase in utilization rate,
though worthy of notice, does not tell us what we most need to know: why this
increase, and is all of it reasonable and proper?
xxix. The public debate over these drugs has tended to use
Ritalin as the generic name for the entire class of stimulants, although
Adderall has actually been the most widely prescribed and used of these drugs
since at least 1999.
xxx. Notwithstanding this conclusion, there has been much
recent discussion about “adult ADHD,” and pharmaceutical companies are
aggressively advertising remedies for this “disorder” on television.
xxxi. In this respect, too, the behavioral disorders being
treated may be seen as paradigmatic. For very few behavioral disorders is there
likely to be a purely genetic cause.
xxxii. Dr. Lawrence Diller, a pediatrician specializing in
behavior problems whose referral practice gets mostly hard-to-diagnose cases,
estimates that in his experience less than half of the children for whom he
prescribes Ritalin are genuine cases of ADHD. See Diller, L., “Prescription Stimulant
Use in Children: Ethical Issues,” presentation to the President’s Council on
Bioethics (www.bioethics.gov), Washington, D.C., 12 December 2002. If
diagnostic difficulties obtain even where experienced and careful experts spend
several hours, involving separate visits also to school and home, to evaluate
the child, one can readily see the risks of misdiagnosis where evaluation is
made during a 10-15 minute visit to the family doctor’s office.
xxxiii. A recent study of the use of stimulants to treat children
for ADHD in a rural North Carolina community is instructive. The authors found
that about a quarter of children with unequivocal symptoms of ADHD were not
receiving stimulant medication. Girls and older children with ADHD were less
likely to receive such treatment. On the other hand, the authors also found
that most of the children receiving stimulants did not actually meet the
diagnostic criteria for ADHD and had never been reported by their parents as
having impairing ADHD symptoms. The authors concluded that, at least in this
community, stimulants were being used in ways “substantially inconsistent with
current diagnostic guidelines”—underprescribed in some cases and overprescribed
in others. (Angold, A., et al., “Stimulant treatment for children: A community
perspective,” Journal of the American Academy of Child and Adolescent
Psychiatry 39: 975-984, 2000.) Commenting on the North Carolina study, Dr.
Benedetto Vitiello of the National Institute of Mental Health emphasized that “research
is urgently needed to elucidate the most common pathways leading to children’s
referral, diagnosis and treatment” (loc. cit., pp. 992-994).
xxxiv. We lack comparable data for other countries. In his
presentation to the Council, Dr. Lawrence Diller reported that the United
States uses 80 percent of the world’s Ritalin. See Diller, L., “Prescription
Stimulant Use in Children: Ethical Issues,” presentation to the President’s
Council on Bioethics (www.bioethics.gov), Washington, D.C., 12 December 2002.
xxxv. Thus, the effectiveness of Ritalin and similar drugs in
calming rowdy children or concentrating unfocused minds does not prove that
those being treated have ADHD.
xxxvi. In 1990, Congress passed the Individuals with Disabilities
Education Act (IDEA), which mandates special education and related services for
(among others) children diagnosed with ADHD. Compared to other alternatives,
according to Dr. Lawrence Diller, “savvy parents prefer to win IDEA eligibility
for their child; it offers a wider range of options, access to
special-education classrooms and programs that are guaranteed funding, and
stricter procedural safeguards.” (Diller, L., Running on Ritalin: A
Physician Reflects on Children, Society and Performance on a Pill, New
York: Bantam Books, 1998, p. 149.)
xxxvii. In addition, a doctor’s diagnosis of ADHD (or
learning disability) will permit college-bound students extra time in taking
the all-important SAT exam, and, since 2001, without any notice of this fact
reported with the results. It will be interesting to discover whether more
students now declare themselves victims of ADHD, eligible not only for extra
time on exams but also for stimulant drugs that could improve their attention
and performance. Already the annual production quotas for Ritalin almost
tripled between 1992 and 1995 (and doubled again between 1995 and 2002). The
2002 quota of 20,967 kg is sufficient to produce a little over one billion
Ritalin pills containing 20 mg of methylphenidate.
xxxiii. Special safety concerns have been raised about the growing
practice of prescribing stimulants “off label” to toddlers as young as two
years old. One concern is that, between the ages of two and four, the brains of
children are still undergoing important biological development that might be
adversely affected by the use of psychotropic drugs. At present, stimulants are
approved by the FDA only for treatment of children age six and above. The
National Institute of Mental Health is currently sponsoring a large study of
the safety and efficacy of stimulants among preschoolers who exhibit ADHD-like
behavior. See Coyle, J., “Psychotropic drug use in very young children,” Journal
of the American Medical Association 283(8): 1059–1060, 2000, and Vitiello,
B., “Psychopharmacology for young children: Clinical needs and research
opportunities,” Pediatrics 108(4): 983-989, 2001.
xxxix. We say “seemingly,” for there may be reasons to
question or doubt whether the use of stimulants by normal, healthy, or even
above-average children would in fact improve performance in the ways that
matter most, or whether the drugs might enhance certain powers and faculties at
the expense of other powers and faculties. As far as we know, there have been
no major studies on the long-term effect of sustained stimulant use simply as a
performance-enhancer or behavior-improver. There is evidence that stimulants do
improve performance in immediate and specific tasks such as test-taking. But
this is hardly sufficient evidence of long-term educational benefit.
xl. The phrase “social control” may raise for some readers
the specter of Soviet-style oppression masquerading as psychiatry. We imply no
such prospect. Yet even without any government policy, people often act to
control the social behavior of children. Drugs offer them a new and potentially
powerful way to do so. Our discussion in this section considers the whole
panoply of behavior-modifying drugs, not just stimulants.
_____________
Endnotes
1. Glass, B., “Science: Endless Horizons or Golden Age?” Science
171: 23-29, 1971, and Sinsheimer, R., “The Prospect of Designed Genetic Change,”
Engineering and Science Magazine, California Institute of Technology,
April 1969.
2. Chan, A., et al., “Foreign DNA transmission by ICSI: injection
of spermatozoa bound with exogenous DNA results in embryonic GFP expression and
live rhesus monkey births,” Molecular Human Reproduction 6(1): 26-33,
2000.
3. Schatten, G., “Assisted Reproductive Technologies in the
Genomics Era,” Presentation at the December 2002 meeting of the President’s
Council on Bioethics, Washington, D.C. Transcript available on the Council’s
website at www.bioethics.gov.
4. Silver, L., Remaking Eden, New York: Avon, 1998, and
Stock, G., Redesigning Humans: Our Inevitable Genetic Future, New York:
Houghton Mifflin, 2002.
5. Enge, M., “Ad Seeks Donor Eggs for $100,000, Possible New High,”
Chicago Tribune, 10 February 2000.
6. Marshall, E., “Gene Therapy a Suspect in Leukemia-like Disease,”
Science, 298: 34, 2002, and “Second Child in French Trial is Found to
Have Leukemia,” Science, 299: 320, 2003.
7. Collins, F., “Genetic Enhancements: Current and Future
Prospects,” Presentation at the December 2002 meeting of the President’s
Council on Bioethics, Washington, D.C. Transcript available on the Council’s
website at www.bioethics.gov.
8. Mandavilli, A., “Fertility’s new frontier takes shape in
the test tube,” Nature Medicine 9(8): 1095, 2003.
9. Pinker, S., “Human Nature and Its Future,” Presentation at
the March 2003 meeting of the President’s Council on Bioethics, Washington,
D.C. Transcript available on the Council’s website at www.bioethics.gov.
10. Hübner, K., et al., “Derivation of oocytes from mouse
embryonic stem cells,” Science 300(5620): 1251-1256, 2003.
11. The President’s Council on Bioethics, Human Cloning
and Human Dignity: An Ethical Inquiry, Washington, D.C.: Government
Printing Office, 2002. The relevant discussion is found in Chapter Five, “The
Ethics of Cloning-to-Produce-Children,” pp. 87-99.
12. Human Reproduction Update, 8(3): 65-277, 2002.
13. Schatten, G., 2002, op. cit.
14. Eberstadt, N., “Choosing the Sex of Children: Demographics,”
Presentation at the October 2002 meeting of the President’s Council on
Bioethics, Washington, D.C. Transcript available on the Council’s website at
www.bioethics.gov.
16. The earliest of these are Assessing Biomedical
Technologies: An Inquiry into the Nature of the Process, Committee on Life
Sciences and Social Policy, National Research Council/National Academy of Sciences,
Washington, D.C., 1975; and Powledge, T. M. and J. C. Fletcher, “A Report from
the Genetics Research Group of the Hastings Center, Institute of Society,
Ethics, and Life Sciences,” New England Journal of Medicine 300(4):
168-172, 1979.
17. President’s Commission for the Study of Ethical Problems in
Medicine and Biomedical and Behavioral Research, Screening and Counseling
for Genetic Conditions: A Report on the Ethical, Social, and Legal Implications
of Genetic Screening, Counseling, and Education Programs, Washington, D.C.:
Government Printing Office, 1983, pp. 57-58.
19. Davis, D., Genetic
Dilemmas: Reproductive Technology, Parental Choices, and Children’s Futures,
New York: Routledge, 2001, p. 98.
20. The Ethics Committee of the ASRM, “Sex Selection
and Preimplantation Genetic Diagnosis,” Fertility and Sterility, 72: 4,
1999.
21. The Ethics Committee of the ASRM, “Preconception Gender
Selection for Nonmedical Reasons,” Fertility and Sterility, 75: 5, 2001.
22. See Hardin, G., “The Tragedy of the Commons,” Science
162: 1243-1248, 1968.
23. The Ethics Committee of the ASRM 1999, op. cit.
24. President’s Council on Bioethics, Human Cloning and
Human Dignity: An Ethical Inquiry, op. cit.
25. Riddle, M., et al., “Pediatric Psychopharmacology,” Journal
of Child Psychology and Psychiatry 42(1): 73-90, 2001.
26. Zito, J., et al., “Psychotropic Practice Patterns for
Youth: A 10-Year Perspective,” Archives of Pediatric and Adolescent Medicine
157: 17-25, 2003.
27. Diller, L., “Prescription Stimulant Use in American
Children: Ethical Issues,” Presentation at the December 2002 meeting of the
President’s Council on Bioethics, Washington, D.C. Transcript available on the
Council’s website, www.bioethics.gov.
28. Rapoport, J., et al., “Dextroamphetamine: its cognitive and
behavioral effects in normal and hyperactive boys and normal men,” Archives
of General Psychiatry 37: 933-943, 1980.
29. Bradley, C., “The Behavior of Children Receiving Benzedrine,” American Journal of Psychiatry 94: 577-585, 1937.
30. Castellanos, F., et al., “Neuroscience of Attention
Deficit/Hyperactivity Disorder: The Search for Endophenotypes,” Nature
Reviews Neuroscience 3: 617-628, 2002.
31. Smalley, S., et al., “Genetic linkage of
attention-deficit/hyperactivity disorder on chromosome 16p13, in a region
implicated in autism,” American Journal of Human Genetics 71: 959-963,
2002.
32. Diagnostic and Statistical Manual of Mental Disorders,
Fourth Edition, Text Revision,
Washington, D.C.: American Psychiatric Association, 2000, p. 93; see also the
appendix to this chapter.
33. Barbaresi, W. J., et al., “How common is attention-deficit/hyperactivity
disorder? Incidence in a population-based birth cohort in Rochester, Minnesota,”
Archives of Pediatric and Adolescent Medicine 156: 217-224, 2002.
34. United States Drug Enforcement Administration, Methylphenidate/amphetamine
yearly production quotas. Washington, D.C.: Department of Justice, 2000.
35. Zito, J. M., et al., “Trends in the prescribing of
psychotropic medications to preschoolers,” Journal of the American Medical
Association, 283: 1025-1030, 2000.
37. See, for example, Eberstadt, M., “Why Ritalin Rules,” Policy
Review 94, April/May 1999; DeGrandpre, R., Ritalin Nation: Rapid-Fire
Culture and the Transformation of Human Consciousness, New York: Norton,
1999; and Hancock, L., “Mother’s Little Helper,” Newsweek, 18 March
1996.
38. Biederman, J., et al., “Pharmacotherapy of
Attention-Deficit Hyperactivity Disorder Reduces Risk for Substance Use
Disorder,” Pediatrics 104: e20, 1999.
39. Elliott, C., Better Than Well, New York: Norton,
2003, pp. 257-258.
40. Hyman, S., “Pediatric Psychopharmacology,” Presentation
at the March 2003 meeting of the President’s Council on Bioethics, Washington,
D.C. Transcript available on the Council’s website at www.bioethics.gov. Dr.
Hyman concluded his presentation to the Council with these remarks.
==============================
Chapter
3. Superior Performance
Human beings desire not only “better children,” we desire
also to be better ourselves. Aspiration, born of the attractiveness of some
human good and the energizing awareness that we do not yet possess it, is at
the heart of much that we do and much that is admirable about us. We strive to
be better human beings and citizens, better friends and lovers, better parents
and neighbors, better students and teachers, better followers of our faiths.
Many of us aspire also to excel in the specific activities to which we devote
ourselves; and nearly all of us admire superior performance whenever we
encounter it, even in areas where we ourselves are only mediocre.
Superior performance is pursued in a myriad of human
activities. The athlete strives to run faster, the student to know more, the
soldier to shoot more accurately, the vocalist to sing more musically, the
chess-player to play with greater mastery. Our motives for seeking superior
performance are varied and complex, as human desire and human aspiration always
are. We seek to win in competition, to advance in rank and status, to increase
our earnings, to please others and ourselves, to gain honor and fame, or simply
to flourish and fulfill ourselves by being excellent in doing what we love. In
pursuing superior performance, human beings have long sought advantages
obtainable from better tools and equipment, better training and practice, and
better nutrition and exercise. Today, and increasingly tomorrow, we may also
find help in new technological capacities for directly improving our bodies and
minds—both their native powers and their activities—capacities provided by
drugs, genetic modifications, and surgical procedures (including the
implantation of mechanical devices). What should we think about obtaining
superior performance through the use of such biotechnologies? That is the theme
of this chapter. But before turning to the question raised by the novel means,
we must begin with questions about the goal itself: “What is superior
performance?”
I. The Meaning
Of “Superior Performance”
The words themselves—”superior performance”—have many
meanings, both individually and together, each of them suggestive and
important. “Superior” can mean “better than I have done before,” or “better
than my opponent,” or “better than the best.” It can describe something that is
universally or indisputably outstanding or something that is better only in
relation to the alternatives. It can also mean—and this is especially relevant
in this context—”better than I would have done without some ‘extra edge’ or ‘performance
enhancement.’” Because superiority, on whatever meaning, is time-bound and
precarious, we not only seek to do better than we have done before. We also
seek to maintain abilities that seem to be slipping away and to regain powers
and abilities that we have lost. We want to become superior and stay superior.
Even more central to our analysis is the meaning (or
meanings) of “performance.” It denotes the active doing of what we do
and the active expression of what we are: living embodied beings
or agents, individually at-work in the world. To be alive at all means that
certain organic systems are performing their functions. In the human
case, active performance includes not only the autonomic activity of a well-working
organism functioning without conscious choice and direction (for example, in
heart beating, digesting, and normal breathing). It also includes the
self-directed performance of various chosen human activities (for
example, walking, running, dancing, thinking). To “perform” an activity
is not just to do it, but to do it thoroughly, “through and through,” to do it
to completion and fullness. The idea of performance also suggests a
relationship with other performers and spectators: performance before others,
with others, and against others. Yet it is also possible to perform certain
activities without others, on one’s own and for oneself, manifesting who
we are for our own enjoyment alone. Temporally speaking, a performance is both
that which is done “in-the-moment” (a great shot to win the game, a great
musical performance) and that which is done “over time” (a great career,
writing a great symphony). It embraces that which is done effortlessly or
seemingly effortlessly (Joe DiMaggio swinging the bat) and that which is done
with great and obvious exertion (Pete Rose hustling to turn a single into a
double). Finally, and most pertinent to this inquiry, the word “performance”
sometimes means a brilliant illusion, a skilled simulation of reality, or the separation
of what one does from who one is: performance as the make-believe acting of
actors rather than the self-revealing doings of genuine doers. “Performance”
suggests both real activity and real agency, but also the possibility of being
or seeming to be something other than who and what we are.
At the core of the notion of “superior performance”—understood
as an object of noble aspiration—is the idea of excellent human activity:
excellent, not inferior; human, not inhuman or nonhuman; active and not
passive, at-work and not idling. The reason we spend much of our lives trying
to “better ourselves”—not just materially, but as athletes, musicians,
soldiers, or lovers—is that we know or believe that not all performances are
equal: some are higher and some are lower, some are more worthy and some are
less worthy, some are excellent and some are average. But we desire to excel as
human beings; we want to exercise our distinctively human powers both
excellently and in our peculiarly human way. We know or believe that some
performances will reveal who we are capable of being when we are at our best.i
The striving for superior performance is, as noted, central
to our humanity. But it also raises a series of questions and dilemmas, and
sometimes unease and concern, not only about the means we employ, but also
about the goal itself. We worry that the desire to become better could deform
elements of human life that are not properly measured according to the standard
of “superiority,” or that our improvements will be achieved only at the price
of our integrity and dignity. We worry that pressures to excel will
overwhelm us, or that the desire to be the best will tempt us to “cheat” our
way to the top. We worry that putting such a high premium on excellence will
crowd out the disadvantaged, or lead us to mistreat those who are “failures.”
In short, we worry about balance, fairness, and charity—but also, and perhaps
more profoundly, we worry about pursuing the wrong goals in the wrong way, or
posing as something we are not.
These enduring questions about the pursuit of superior
performance acquire heightened visibility and greater salience as a result of
emerging new biotechnological powers, present and projected, that promise to
help us in our efforts. These powers are surgical, genetic, and
pharmacological. Some are familiar—like steroids used to enhance athletic
performance and amphetamines used to enhance mental performance. Others are
novel—such as the genetic modification of human muscles. And still others are
imaginary rather than real—such as genetically engineered Michael Jordans or
drugs that would give us perfect memory.
Most of the performance-enhancing technologies of the
future, like those in use today, will probably be developed less to aid
superior performance than to treat disease and relieve suffering. Yet the broad
powers of many drugs and devices make them readily adaptable to uses for which
they were not originally intended. Our biotechnical armamentarium for aiding
superior performance is still extremely limited. Yet we are already witnessing
the wide range of activities that might be biologically enhanced. Modafinil, a
drug that combats narcolepsy and induces wakefulness more generally, has been
shown to enhance the performance of airplane pilots, commercial and military.
Ritalin, the amphetamine-like stimulant whose use in children we discussed in
the previous chapter, is also widely used by high school and college students
to improve their concentration while taking the SATs or writing final exams.
Viagra, a remedy devised for male impotence, is increasingly used by the
non-impotent to enhance sexual performance. Growth hormone, the body’s natural
promoter of skeletal growth, is now being used not only to treat dwarfism but
also to help the normally short to become taller. Other drugs are used to calm
the nerves or to steady and dry the hands of neurosurgeons and concert
pianists. These examples constitute but a small preview of coming attractions.
To fully understand the meaning of using these new
biotechnical powers, in all their variety of effects and possible uses, we
would need to inquire more deeply into the meaning of “superior performance”
itself. We would need to explore the reasons we seek to become better, the
abilities we seek to enhance, the different means we might use to enhance them,
and the true character of the different activities in which we engage. We would
need to pay attention both to the ends we seek and the means and manner by
which we seek them, as well as the differences between given human activities,
their various excellences and what it takes to attain them. And, attending to
the special issues raised by the use of bio-engineered enhancements, we
would need to address these central questions: As we discover new and better
ways to “improve” our given bodies, minds, and performance, are we changing or
compromising the dignity of human activity? Are we becoming too reliant on “expert
chemists” for our achievements? Do such potential enhancements alter the
identity of the doer? Whose performance is it, and is it really better? Is the
enhanced person still fully me, and are my achievements still
fully mine? Have I been enhanced in ways that are in fact genuinely better
and humanly better? And, beyond these questions regarding individuals,
we would need to consider the implications for society should such uses of
biotechnology become widespread—in school, at work, or in athletics, warfare, or
other competitive activities.
Needless to say, such a comprehensive examination is beyond
the possible scope of this discussion. There are too many different kinds of
superior performance and too many conceivable biotechnical means of enhancing
the performers. To introduce the subject and to illustrate the ethical and
social issues involved, we confine ourselves largely to one particular case
study in one particular area of human activity: human sport. It is an activity
where human excellence is both recognizable and admired, where concerns about
wrongfully enhancing performance are familiar, and where disquiet about the use
of “performance-enhancing drugs” is widely shared if not always fully
understood. As we shall see, many of the larger questions readily emerge from
this case study, and the relevance of the present analysis for other human
activities should be plain. Where explicit comparisons with other human
activities will prove revealing, we shall not hesitate to bring them into the
picture.
II. Sport And
The Superior Athlete
A. Why Sport?
At first glance, focusing on athletic excellence may seem
strange. True, sports are hugely popular and exciting, and the achievements of
our greatest athletes are very impressive. But is sport important? Why spend
time worrying about the dignity of athletics when there are many more serious
problems in the world and when many life and death dilemmas in bioethics are so
pressing? Such questions raise a powerful point: many aspects of human life are
indeed more significant or more worth worrying about than athletics.
Nevertheless, if one is interested not only in combating human misery but also
in promoting human excellence, the world of sport is an extremely useful case
study. Indeed, what we learn of wider application from thinking about athletics
may prove far more significant than it first appears.
For one thing, sport is an area of human endeavor where
human excellence is widely admired—where we honor the best for their
achievements, and where we admire the striving of those who seek to improve,
achieve, and excel.ii
Athletic excellence appeals partly because it is open, genuine, and publicly
visible, inviting thousands of otherwise disconnected individuals to unite in
shared appreciation. In perhaps no other contemporary activity is there such a
manifestly evident and celebrated display of individual (and group) human
excellence.
Second, sport is an activity that invites deeper reflection
about our bodily nature, and especially our distinctly human bodily nature.
After all, animals and machines can do many things much better than we
can—artificial pitching machines can “throw” harder, cheetahs can run faster.
But it is the human athlete that we admire. Understanding why this is so has
implications far beyond athletics.
Third, sport is an area of life where we have made some
effort—both cultural and legal—to preserve the “dignity of the game,” so to
speak, from “cheating,” both biological (for example, steroids) and mechanical
(for example, corked bats). But we have done so without always examining
precisely how the dignity of the game or the excellence of the performance
would be compromised were the use of these enhancing agents to become normal.
Thus, while we begin this analysis by acknowledging that “life
is not a game,” we also suggest that things essential to sport—such as
aspiration, effort, activity, achievement, and excellence—are essential also to
many aspects of the good human life.iii
Examining the significance of performance-enhancing biotechnical powers for
human sport may help us understand the significance of such powers for
excellent human activity more generally.
B. The Superior Athlete
To be a superior athlete depends on numerous things: native
gifts, great desire, hard work, fine coaching, worthy competitors, sound
equipment, good luck. The types of talents needed will vary with the sport or,
in team sports featuring specialization, with one’s position or role. But any
superior athlete requires strength, drive, endurance, coordination, agility,
vision, quickness, cleverness, discipline, and daring, shared virtues of body
and soul that manifest themselves in different ways and degrees depending on
the activity and the way one performs it. And, in every sport, at every level
of competition, superior performance matters.
Some ways of becoming a superior athlete center on the
athlete himself: for example, healthy physical growth, better training, more
experience. Others involve outside help: better coaches, better teammates,
better competitors. Some involve improving one’s equipment: fiberglass vaulting
poles, graphite tennis rackets, high-tech high-tops. And others involve
improving one’s own body: high-protein diets, vitamin supplements, anabolic
steroids, genetic modifications. These different approaches can be
complementary or overlapping: better diet improves one’s capacity to train, and
better training improves one’s body and its powers. We intuitively sense,
however, that there may be a difference between, for example, lifting weights,
eating egg whites, and using a graphite tennis racket, just as there appears to
us to be a difference between eating egg whites and taking anabolic steroids.
But if so, understanding the true nature and significance of these differences
is a complex matter, not easily specified. How do the different means of
becoming superior differ from one another? Is the excellence or superiority of
an activity affected by the way it is done or pursued? Do some ways of
improving performance change the actual character of the activity? If some
performance enhancements are considered “cheating,” just who or what is being
cheated—one’s competitors, one’s fans, oneself, or the dignity of the activity
itself? These are the sorts of questions we shall try to answer.
C. Different Ways of Enhancing Performance
As already indicated, there are multiple ways to improve
athletic performance, from the elementary to the sophisticated, from the old to
the new. Consider, for example, competitive running. The ancient Greek runners
ran barefoot. Then the use of shoes protected against injury. Cleats gave
greater traction. Better nutrition augmented general health and energy. Weight
training strengthened muscles. Regimens of practicing wind sprints or
fixed-distance runs built up endurance. Competition during training provided
motivation and experience. Coaching improved mechanics and strategy. High-tech
shoes improved efficiency of motion. Erythropoietin injections increased oxygen
carrying capacity. Anabolic steroids permitted greater weight training leading
to enlarged muscle mass. Stimulant drugs aided alertness and concentration.
Someday, insertion of synthetic muscle-enhancing genes may make muscles
stronger, quicker, and less prone to damage.iv
Where in this sequence of devices to improve running do we acquire any disquiet
regarding the means used? Why, if we are disquieted, are we bothered?
To prepare for the answers to these questions, let us look
more closely at a number of different ways of improving athletic performance—some
celebrated and some not, some already here and some on the horizon. They fall
generally into three categories: better equipment, better training, and better
native powers.
1. Better Equipment.
Examples of superior performance through better equipment
are ubiquitous. Pole-vaulting used to be done with rigid bamboo poles and
vaults of fifteen feet high seemed virtually superhuman; now flexible
fiberglass poles are used, and vaults go over nineteen feet. Baseball gloves
were once little more than shaped padding for the hand; now, more than twice
their original size, they resemble small bushel baskets. Curved hockey sticks,
replacing the straight ones, make possible greater puck control and faster
shots. Graphite tennis rackets yield greater racket speed and power. With such
equipment now an accepted part of the sport, used by virtually everyone in
competitive and professional athletics, players who did not use them would be
looked upon as foolish, and they would likely never make it to the highest
levels of competition.
Yet not all performance-enhancing equipment is welcomed
into sport. Corked baseball bats, for example, are believed to permit increased
bat speed and thus hitting power. Yet they are considered an unacceptable form
of cheating and are illegal in professional baseball. Players who use them are
looked down upon by many fans as “cheaters” or seen as fools for believing they
could get such an unfair advantage without getting caught. Were someone to
propose that the rules be changed, so that everyone could use corked bats, many
people would probably still object. Owing to the importance of history and
statistics in the glamour of baseball and the desire of fans to be able to make
valid comparisons of superior performance across the generations, their wish to
see more home runs does not—at least for now—trump their wish to preserve the “integrity
of the game.” Comparing graphite tennis rackets (which we embrace) and corked
baseball bats (which we decry) suggests how our objections to performance-enhancing
equipment are often conventional, with differences due to traditions, chance
histories, or elective decisions about the rules of the game. Some of these
rules are not matters of principle but of taste, while others involve
particular discernments about what is best for individual sports that cannot be
universalized.
2. Better Training.
Better training can take several forms. It could become
more rigorous, the athlete working harder and longer than he did before or
harder and longer than his teammates or his rivals. Training could be more
effective (better, not necessarily harder), the athlete training more
intelligently or scientifically. And training could be better coached, the
athlete practicing under the guidance of someone with superior wisdom or
know-how regarding nutrition, general fitness, or specialized skills such as
batting or pitching.
All of these forms of improving performance through
training proceed through habituation, practice, and instruction, consciously
and conscientiously undertaken. Yet the effects of the training are often
written into the bodies of the athletes, in the form of increased strength,
longer endurance, greater quickness, improved coordination, and smoother
performance. Similar bodily changes might also be produced not through active
training or active training alone, but by direct biotechnical intervention into
the body of the athlete, seeking to improve his native capacities by altering
his underlying genetic or biochemical make-up.
3. Better Native Powers.
Direct biological means of improving the powers of our
bodies range from the small and familiar to the large and novel. Least dramatic
are special diets, for example, diets high in protein, known for decreasing
body fat and increasing muscle mass. There is laser eye surgery to correct
imperfect or “low-performing” eyesight, capable of producing permanent
improvements in the patient’s vision with a single treatment. Some prominent
athletes (including Tiger Woods) have used this surgery to get “better-than-normal”
eyesight, a practice that is fully legal and considered by all professional
sports to be an acceptable “enhancement.”
More invasive, more controversial, and (for now) illegal in
competitive athletics are the uses of various drugs to enhance performance:
stimulants like amphetamine to produce heightened attention and quicker
reactivity; erythropoietin (EPO) to overproduce red blood cells and, hence, to
augment the body’s carrying capacity for oxygen (so-called “blood doping”);
human growth hormone to increase height or generalized vigor; and anabolic
steroids to facilitate training that will increase overall muscle mass. Off in
the future, but already visible on the drawing board, are prospects of genetic
enhancement of bodily strength and resilience through the insertion into
muscles of genes for erythropoietin or more specific muscle growth factors.
Because so much of athletic excellence is based on strength and swiftness, the
muscle-enhancing technologies are under special scrutiny by the sports authorities.
They are also of special interest to us. To illustrate how present and
prospective biotechnologies can enhance native bodily powers, we turn next to
various technological approaches to direct muscle enhancement, both
pharmacologic and genetic.
III. Muscle
Enhancement Through Biotechnology
A. Muscles and Their Meanings
Our muscles are essential to human life in many ways. They
are central agents of physical strength and speed, attributes admired and
celebrated in most human cultures. All of our motions—from walking, swimming,
and lifting, to writing, chewing, and shaking hands—depend on them. As basic
elements of physicalvigor, they also play a role in human attractiveness and in
our sense of well-being and even our sense of who we are. Our path through the
life cycle is displayed most vividly in the changes of our musculature.
When we are young, the active use of our muscles in play
and in sports strengthens and develops them. At puberty, production of estrogen
and testosterone enhances these processes, so that the peak of human muscular
development usually occurs between ages 20 and 30. Thereafter, the strength and
size of human muscles usually declines, falling off by about one-third between
the ages of 30 and 80.1
As we age, we gradually lose the ability to dovarious physical tasks, sometimes
in part, sometimes altogether.v
There are, of course, individual variations from this
general pattern. Some people suffer from muscle diseases, often caused by
specific genetic mutations (for example, muscular dystrophy), that render them
unable to develop their muscles to the same extent as the healthy. Others
manage through exercise and fitness training to maintain peak muscular strength
and endurance much longer than the average. Still others, sedentary and
inactive, neglect those maintenance functions altogether and fall weaker
earlier than most.
Muscles do not generate human strength and speed in
isolation. They need to be physically integrated with, and function
harmoniously through their attachments to, nerves, tendons, ligaments, and
bones. While our attention will be on enhancing the activities of muscles and
their cells, this fact reminds us that any biotechnological intervention that
strengthens only muscles may unbalance the interactions with these other body
parts, with serious malfunction as a possible consequence.
Though not exactly a matter of athletic performance, the
perfection of our musculature and body build is a matter of great concern to
many people intent on improving their body image. Muscles have always played a
prominent role in the idealizations of male human form. A classical picture of
excellence of the youthful male human form is Michelangelo’s sculpture of
David, completed around 1504. The musculature is well developed and well
proportioned but without much articulation of individual muscles; indeed, the
integrated physique points not to itself but to some impending action. Yet
David’s strength and power shine through the marble, and leave us with a mental
picture of the classical ideal of muscular development and proportion, poised
for graceful and superior performance.
A more contemporary idealization of the male human form is
the modern bodybuilding champion, such as Arnold Schwarzenegger. Through
specialized weight training, perhaps with the help of anabolic steroids, all
the muscles (especially the biceps and pectoral muscles) become much larger
than those in the statue of David, and the different groups of skeletal muscles
are individually articulated. The picture is less one of measured and
proportionate strength in the service of splendid activity, more one of “muscle-bound”
power, to be admired for its own sake.vi
Yet although they differ in proportion and muscle articulation, both the
classical and contemporary ideals testify to the importance of muscles in
images of male strength and power.vi
The body’s appearance reveals more than a superficial
image. As embodied agents of our innermost will, muscles not only work our
purposes on the world, but make manifest the deep qualities of our character,
our dispositions and intentions, our self-discipline, self-development, and
self-image. We are highly attentive to posture and motion in others, and
muscular actions make possible the communication and cooperative coordination
essential for human society. All of these qualities are especially evident—and
therefore visible for evaluation—in many forms of athletic performance.
B. Muscle Cell Growth and Development
Scientists have learned a great deal about the cellular
structure and development of skeletal muscles, as well as about how genes
important to muscle cells function and are regulated. The following brief
discussion of muscle cell biology will reveal targets for biotechnical
interventions aimed at improving muscle strength and resilience.
The major cell type present in skeletal muscle fibers is
the multinucleated myotube, a long cylindrical cell that does the contracting.
These myotubes arise from precursor cells, mononucleated myoblasts, by means of
their fusion with each other and with pre-existing myotubes. Myoblasts, in
turn, are formed by differentiation of a particular stem cell found in muscle
tissue, called a satellite cell.2
The multiplication and differentiation of satellite cells
into myoblasts is regulated by several specific protein growth factors
(primarily insulin-like growth factor 1 [IGF-1] and hepatocyte [liver cell]
growth factor [HGF]). This process is also influenced by hormones such as
growth hormone, testosterone, and estrogen. Growth hormone secreted by the
pituitary acts on the liver to stimulate synthesis of IGF-1 and its subsequent
release into the circulation. (See Figure 1.)
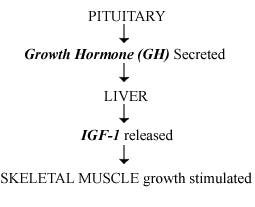
Figure 1. Hormone action and muscle growth stimulation.
In muscle tissue, IGF-1 binds to specific receptors on the
surface of satellite cells to stimulate their multiplication, producing both
differentiation of satellite cells into myoblasts as well as more satellite
cells. (See Figure 2.)
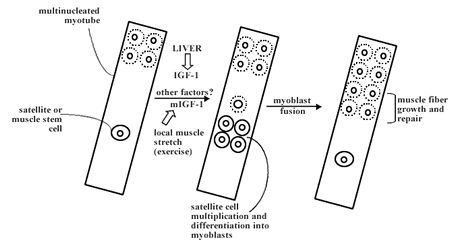
Figure 2. Schematic diagram of some important processes in skeletal muscle fiber growth and repair.
Importantly, a slightly different form of IGF-1 (muscle
IGF-1 or mIGF-1) is also produced locally in muscle tissue in response to
stretching the muscles during exercise. This form is thought to act the same
way as circulating IGF-1 does in stimulating satellite cell multiplication and
differentiation. However, because mIGF-1 is slightly different in chemical
structure from IGF-1 produced in the liver, mIGF-1 apparently does not enter
the circulation, so its effects can be restricted to promoting growth and
repair of muscle tissue locally.
C. Opportunities and Techniques for Muscle Enhancement3
We can now see how attempts at muscle enhancement might
work. As has long been known, exercise increases muscle size and strength.
Exercise both transiently damages muscles and, in response, causes them to
increase in size and strength. Exercise (muscle stretch) increases the
production of a specific locally active form of insulin-like growth factor
(mIGF-1), a major mediator of muscle stem cell growth and differentiation. As a
consequence of IGF-induced stimulation, muscle stem (satellite) cells multiply,
differentiate, and fuse. As a result, the number of muscle fibers increases.
Biotechnological research and development have introduced
new possibilities for producing similar muscle proliferation and enhancement,
both genetic and pharmacological. The genes for animal and human IGF-1 have
been cloned and their DNA sequences determined. Gene expression vectors have
been developed that permit the regulated production of IGF-1 proteins (both the
liver and muscle forms) for investigation. Thus IGF-1 genes can be introduced
into cells and experimental animals—for example, by means of viral vectors—to
determine the effect of enhanced IGF-1 (or mIGF-1) production on muscle size
and strength. Recent experiments along these lines in animals have yielded very
exciting results.
For example, in experiments described by Barton-Davis and
coworkers,4
recombinant virusesviii
containing a rat IGF-1 gene were injected into the anterior compartment of the
rear legs of young mice containing the extensor digitorum longus (EDL) muscle.
The resulting increased production of IGF-1 promoted an average increase of
about 15 percent in EDL muscle mass and strength in young adult mice.
Strikingly, such injections led to a 27 percent increase in the strength of the
EDL muscles when the mice approached the average lifespan of 27 months. In
fact, the continued presence of additional (rat) IGF-1 genes essentially
prevented the decline in muscle size and strength observed in untreated old
mice.ix x
An alternate route to genetic enhancement exploits the
ability, at embryonic stages of development, to create transgenic animals in which
an appropriately regulated foreign gene is expressed throughout embryonic and
adult life. Musaro and his colleagues5
introduced a rat mIGF-1 gene into early-stage mouse embryos, where it became
integrated with mouse chromosomal DNA. The resulting transgenic mice produced
substantial amounts of rat mIGF-1, in addition to their own mouse IGF-1 and
mIGF-1. Embryonic development of these transgenic mice proceeded normally. Yet
as early as ten days after birth, the skeletal muscles of the transgenic
animals were enlarged, compared to the non-transgenic control mice. Moreover,
the skeletal muscle enlargement persisted as the transgenic mice aged. Whereas,
in unmodified (wild type) mice, muscle size and strength peaked around six
months and decreased considerably by twenty months of age, the size and
strength of skeletal muscle in the transgenic mice (containing rat mIGF-1)
remained stable at peak levels for up to twenty months.xi
These and other experimental results stimulate thoughts
about possible extensions of these approaches to humans. They hold out the
promise of treatments for various diseases of muscle tissue, for sarcopenia and
the weaknesses of old age, and for generalized enhancement of muscle strength
and fitness in people of all ages, diseased or not. Based on our current
understanding, at least three different approaches could be considered. First,
one could introduce muscle-enhancing genes directly into the muscles
themselves. To do so, one would need to develop recombinant virus vectors
containing the human mIGF-1 gene, under the control of appropriate regulatory
elements that would limit its expression to muscle cells near the site of
injection. Alternatively, one might introduce an appropriately regulated mIGF-1
gene into human embryos, as was done in the experiments with mice. Finally, one
might use an approach that combined techniques of stem cell and genetic
engineering. After isolating and expanding human muscle stem (satellite) cells
in vitro, one could introduce an appropriately regulated human mIGF-1 gene into
those cells and then transplant the genetically modified satellite cells back
into the muscles of the person being treated.
None of these three approaches has yet been tried in human
beings. Each has its advantages and disadvantages.xii
Developing any one of them would take a lot of time and money, and many
technical and logistical problems would need to be overcome before any
treatment could be applied on a large scale. Even before the first genetic
treatments to increase muscle size and strength could be tried in humans in the
United States, the Food and Drug Administration (FDA) would require
demonstrations that the proposed treatment is safe and effective.
Nevertheless, the time may be coming soon for human trials
using the first approach, undertaken not to bulk up aspiring athletes but to
treat human muscle diseases. Clinical trials of regulated mIGF-1 gene delivery
as a treatment for specific forms of muscular dystrophy may begin within the
next several years.6
These clinical trials will likely provide crucial data, en route, on
administration, optimal dose, and possible side effects. If efficacy is
demonstrated and side effects are small, one can easily imagine the social and
economic factors that will favor vast expansions in the use of genetic muscle
treatments to enhance muscle size and strength. High school wrestling and
football coaches, having learned of the enhancing gene transfer experiments in
rats and mice, have already expressed interest in obtaining such treatments for
their athletes. Developing a product for which the eventual potential market is
up to 100 percent of the human population will be hard to resist.
Genetic treatments for increasing muscle size and strength
are still in the future. But pharmacological means of doing so are already here
and in use, and both the desire and the rationale for their use is clear. As
noted earlier, various hormones and growth factors play key roles in
stimulating muscle stem cells to multiply, differentiate into myoblasts, and
then fuse with existing muscle fibers. Growth hormone levels influence the size
and strength of muscles, perhaps through the intermediacy of IGF-1. Testosterone
levels influence muscle size and strength, helping to explain why men’s muscles
are generally larger and stronger than women’s. Finally, local growth factors
like mIGF-1 have important effects as well.
At the present time, three different sorts of drugs are
being used to increase (or try to increase) muscle strength. In the newest
practice, still on a very small scale, people have begun to use human growth
hormone in attempts to enhance muscle size and strength, especially in the
elderly. Now that the patent on human growth hormone has expired (2002), the
cost of the monthly hormone injections is likely to drop from its steep $1,000.
If this occurs, the scale of growth hormone use might very likely increase, as
promotion for new uses grows; over the past year, unsolicited e-mail
advertisements for human growth hormone have come frequently to the e-mail
boxes of Council staff.xiii
Competitive athletes (and others) interested in boosting muscle size and
performance have started using growth hormone—though the data suggest that its
effectiveness is uncertain.7
A second approach to the enhancement of muscle performance
works indirectly, not by enlarging muscle size but by increasing muscle
endurance. Known as blood doping, it was originally accomplished by drawing
blood from athletes, separating and concentrating the red blood cells, and then
re-infusing the red blood cells into the athletes’ bloodstream. This raised the
amount of hemoglobin (the oxygen-binding protein) in the blood, and thus
increased the oxygen-carrying capacity of the blood. Much the same effect can
now be obtained by injections of the synthetic protein hormone erythropoietin,
which stimulates the body to increase its production of red blood cells. For
competitive cyclists, swimmers, and long-distance runners, increased
oxygen-carrying capacity in the blood makes possible increased endurance, which
in turn improves competitive performance.
The most commonly used chemical means of muscle enhancement
are the anabolic steroids, chemical compounds related to hormones like
testosterone. Taken orally (for example, “Anadrol” [oxymetholone], “Winstrol”
[stanozolol], or “THG” [tetrahydrogestrinone]), or by injection (for example, “Durabolin”
[nandrolone] or “Equipoise” [boldenone]), these drugs facilitate bodybuilding.
Used in combination with weight training and special diets, they can greatly
increase muscle size and strength. It is true that the precise benefits of
these drugs for athletic performance are in dispute among scientific
researchers, and, for obvious reasons, we have not seen adequate controlled
studies to clarify their true effects. Nevertheless, many athletes, trusting
their own experience and the testimony of teammates, are not waiting for the
scientific evidence. Despite the known health risks and despite official
opposition from the professional and college athletic authorities, as
information about their effects has diffused throughout American society, more
and more professional and amateur athletes are apparently using them. Also
believing that they are effective—and that they are dangerous to the athletes—anti-doping
sport organizations have banned most of them. At the same time, many (including
the ones listed above) are listed as available for sale on the Internet.
Despite the opposition of Olympic and other sports
officials to their use, the public attitude toward steroid use by athletes may
be changing, at least for sports like baseball, basketball, and football. The
recent outcry regarding Sammy Sosa’s corked bat seemed to exceed any protests
against the multiple revelations of steroid use by professional athletes.
Malcolm Gladwell suggests an explanation:
We have come to prefer a world where the distractible take
Ritalin, the depressed take Prozac, and the unattractive get cosmetic surgery
to a world ruled, arbitrarily, by those fortunate few who were born focused,
happy and beautiful. Cosmetic surgery is not “earned” beauty, but then natural
beauty isn’t earned, either. One of the principal contributions of the late
twentieth century was the moral deregulation of social competition—the
insistence that advantages derived from artificial and extraordinary
intervention are no less legitimate than the advantages of nature. All that
athletes want, for better or worse, is the chance to play by those same rules.8
(Emphasis added.)
It is hard to predict how widely genetic and chemical
agents of muscle enhancement would be used, especially should safer versions be
developed. Given the popularity of bodybuilding and fitness today, one could
imagine that biotechnical agents would be useful for enhancing these
activities, both in competitive and non-competitive settings. The commercial
and competitive pressuresto use genetic muscle treatments to build up,
maintain, and repair the muscles of competitive professional athletes in all
sports would surely be very strong. And since athletic competition extends down
from professional and collegiate ranks to youth soccer and Little League, there
would seem to be no place to draw a line against using (safe) genetic or
chemical muscle treatments. The incentive to use these treatments during
adolescence or young adulthood might increase considerably if it should turn
out that treatment during these earlier times of life is also the best means of
protecting against the sarcopenia of old age.
Thus, it is not too farfetched to imagine that parents may
one day be faced with difficult decisions regarding the development of their
children’s bodily capacities for athletics. What will and should they do when
daughter Jenny’s soccer coach tells them she would be a stronger player if they
got her genetic muscle treatments, or that she is more likely to make the team
if she gets treated? Would untreated children or aspiring athletes become
significantly disadvantaged in a society in which many others had genetic or
chemical muscle treatments? Conversely, would these new technologies at last
provide the remedy for those to whom nature dealt a weaker bodily constitution?
Given the difficulty of setting principled limits between the therapeutic uses
of these new biotechnical powers and the uses that go “beyond therapy,” why
might we still seek to set any limits at all?xiv
What is it that such limits would or should seek to defend? It is none too soon
to begin to think about these questions, for the future that will make them
anything but speculative is now visible on the horizon.
IV. Ethical
Analysis
To begin the ethical analysis, we must try to distinguish
between different ways of achieving superior performance, and how these ways of
becoming better might alter, enhance, corrupt, or perfect our different
activities. For those performance enhancements that we embrace, are we so sure
that they are improvements, if we understand “improvement” to mean enhancing
performance in ways that serve, rather than call into question, the dignity or
excellence of human activity? And for those performance enhancements that
trouble us, what is the nature of our disquiet? Because we want to see the
bigger picture, we deliberately take a general approach to these questions, not
tying our analysis to any specific means of boosting muscle strength and
athletic performance. Rather than spend time on issues peculiar to a particular
technique—say, the special safety concerns of genetic transfer, as contrasted
with those associated with growth hormone or steroid use—we will concentrate on
the larger issues raised by our acquiring and using the new bodily powers that
these techniques, each in its own way, supply or promote.
A. How Is Biotechnical Enhancement Different?
The first task is to try to figure out whether using
biotechnological means to gain superior performance is different from using
better equipment or engaging in better training. If it is, what might the
differences be, and what ethical and social difference do they make? This task
is more difficult than it might at first glance seem, for there are
similarities as well as differences among these three approaches. Some analysts
will try to use such similarities to dismiss expressions of concern regarding
drug-mediated improvements: “How are steroids really different from Air Jordan
basketball shoes? Special diets and drugs both increase the capacity to train,
so why make such a fuss about the drugs?” In response, it is worth emphasizing
in advance that the ethical evaluation of biotechnological enhancements does
not finally depend on their being found utterly unique and unprecedented.
The fact that taking anabolic steroids or using genetic muscle enhancers could
resemble, in some respects, using special diets or special bodybuilding
programs does not by itself dissolve all our moral concerns. On the contrary,
it might lead us to think more deeply about the more familiar modes of seeking
to promote superior performance. Moreover, as we shall see, a careful
examination may reveal that, similarities notwithstanding, the differences are
in fact humanly and ethically significant.
In many areas of life, including sports, we take for
granted that better equipment makes for better performance. Better gadgets,
tools, machines, and devices are both yesterday’s news and tomorrow’s
headlines. We habitually think and act in ways that assume the existence of
such equipment, and in many areas of life, we work endlessly and deliberately
to make cutting-edge improvements in our “high-performance gear.” Unlike
training or drugs that change the agent directly, the equipment that boosts our
performance does so indirectly, yet it does so quite openly and in plain sight.
We can see how the springier running shoes, the lighter tennis racket, and the
bigger baseball glove enable their users to go faster, hit harder, and reach
the formerly unreachable—yet without apparently changing them in their persons
or native powers.
Yet appearances are deceiving. That their effects on our
performance are indirect does not mean that they are trivial. And that they
remain but visible tools in our hands does not mean that we remain in fact
unaltered. Although the alterations, unlike the tools that produce them, are
often hard to see, they often go very deep. Not only do we think and act in
ways that assume enhanced equipment, we come to take its use for granted. Not
only do we come to rely on our better tools; after a while, we have trouble
remembering that we could do without them, largely because in truth we cannot
do without them. This is not to suggest that we should do without them
or that there is something wrong with accepting the extra edge that they give
us in our pursuit of excellence. It is merely to insist that the use of
equipment in sports, as in the rest of life, changes and even binds the human
users, often without their knowing it.
The point was beautifully made by Rousseau, commenting on
how even the earliest human inventors of artful aids to better living “imposed
a yoke on themselves without thinking about it”:
For, besides their continuing thus to soften body and mind,
as these commodities had lost almost all their pleasantness through habit, and
as they had at the same time degenerated into true needs, being deprived
of them became much more cruel than possessing them was sweet; and people were
unhappy to lose them without being happy to possess them.9
(Emphasis added.)
Our gear (like all our technology) not only improves the
way we do things. In the process, it also often changes the very things that we
do. It changes the abilities that matter most, and thus the character of our
aspirations and the economy of social rewards. Once again, this is not to
suggest we should not seek further improvements in our equipment. It is merely
to recognize the far-reaching changes, in us and our activities, that the “merely”
external equipment can cause—in all that we do, not only in sports. Because of
graphite tennis rackets, tennis today is a game of faster serves, stronger
strokes, and shorter points, and in consequence requires players of different
talents and demeanor than it did only decades ago. Similarly, because of
precision-guided weapons and drones, warfare now requires a different and more
technical kind of expertise, often less demanding of, and less rewarding to, the
physical human powers that served best in hand-to-hand combat. And because of
computers, there is a premium on those with habits of mind shaped for
programming; indeed, the very way many people think, speak, and write has
changed to fit with the possibilities and necessities of the computer age.
Adapting Winston Churchill’s sage remark about architecture, we might say that
we shape our equipment and our equipment shapes us.xv
The distinction between better equipment and better
training, and even between better equipment and better native powers, is for
additional reasons not as sharp as one might wish. For some forms of athletic
(and other) equipment are developed not to enhance specific performance as
such, but rather to help individuals change or improve themselves precisely
through better practice or training. For example, state-of-the-art weight
training equipment aims at allowing individuals to make themselves stronger
weightlifters and linebackers; state-of-the-art flight simulators allow
individuals to make themselves better pilots. Such equipment is a tool that
explicitly enables us to change ourselves through our own activity; it is an
indirect means to directed and chosen change. Moreover—and more profoundly—the
line between person and equipment may be eroding: we already have such
therapeutic interventions as artificial limbs and mechanical implants to help
blind people to see and deaf people to hear. Mechanical implants of various
other kinds are no longer matters merely for science fiction.
Nevertheless, as with night and day in relation to
twilight, the blurring of the boundaries between the several approaches does
not make the territories themselves indistinct. We can still separate in our
mind those means of altering or improving performance that work by giving us
tools to perform in new ways, and those interventions that work by changing us
directly—whether through self-directed activity and training or through direct
biological interventions in the human body and mind. We can distinguish using
better sneakers from daily running practice for an upcoming race, and both of
these from running the race with the benefit of EPO or steroids. In addition,
even though our tools change us, they do not necessarily change us
irreversibly. We can, if we wish, still try to play baseball with the small,
soft gloves of yesteryear, or softball with no gloves at all. Despite the
fuzziness at the boundary, it still makes sense to distinguish our tools and
equipment from our practice or training, as well as from the more direct
biotechnical interventions aimed at improving our native bodily capacities.
In athletics, as in so many other areas of human life,
practice and training are the most important means for improving performance,
and superior performance is most generally attained through better training:
the direct improvement of the specific powers and abilities of the human agent
at-work-in-the-world, by means of his self-conscious or self-directed effort,
exercise, and activity. To train is to be at work: striving, seeking, pushing,
laboring, and developing. It requires self-knowledge or external guidance about
the ends worth seeking, and it requires the desire and discipline to pursue
those ends through one’s own effort. And, most importantly for our purposes,
training means acquiring by practice and effort improvements in the very powers
and abilities that training uses. One gets to run faster by running; one
builds up endurance by enduring; one increases one’s strength by using it on
ever-increasing burdens. The capacity to be improved is improved by using
it; the deed to be perfected is perfected by doing it.
This insight has some important implications. First, it calls
our attention to the very real differences in our natural endowments. If
improving through training proceeds as described, certain native abilities are
often a prerequisite. In many cases, no amount of training can overcome the
unchangeable shortcomings of natural gifts. Second, and more important for
present purposes, the source of our different endowments may be mysterious, but
our active cultivation of those endowments, whether great or small, is
intelligible: we can understand the connection between effort and improvement,
between activity and experience, between work and result.
This leads to an important difference between improvements
made through training and improvements gained through bioengineering. When and
if we use our mastery of biology and biotechnology to alter our native
endowments—whether to make the best even better or the below- average more
equal—we paradoxically make improvements to our performance less intelligible,
in the sense of being less connected to our own self-conscious activity and
exertion. The improvements we might once have made through training alone, we
now make only with the assistance of artfully inserted IGF-1 genes or anabolic
steroids. Though we might be using rational and scientific means to remedy the
mysterious inequality or unchosen limits of our native gifts, we would in fact
make the individual’s agency less humanly or experientially intelligible
to himself.
The IGF-1-using or steroid-using athlete surely improves:
he (or she) develops and becomes superior—and certainly the scientist who
produced the biological agents of such improvement can understand in scientific
terms the genetic workings or physiochemical processes that make it possible.
But from the athlete’s perspective, he improves as if by “magic,” without the
self-conscious or self-directed activity that lies at the heart of better
training. True, steroids (or, someday, genetic muscle enhancement) will enable
him to perform at a higher level only if he continues to train. True, as he
trains, he still tires, perspires, and feels his (altered) body at-work. But as
the athlete himself can surely attest, the changes in his body are decisively
(albeit not solely) owed to the pills he has popped or the shots he has taken,
interventions whose relation to the changes he undergoes are utterly opaque to
his direct human experience. He has the advantage of the mastery of modern
biology, but he risks a partial alienation from his own doings, as his identity
increasingly takes shape at the “molecular” rather than the experiential level.
Indeed, the athlete’s likely embarrassment proves the point: Even were steroids
or stimulants to become legal, one imagines that most athletes would rather not
be seen taking their injections right before the race. For there is something
shameful about revealing one’s own chemical dependence right before
demonstrating what is supposed to be one’s own personal excellence.
This is not to suggest that changes in the body produced
through training and effort are not also molecular, or to ignore the fact that
the very purpose of certain biochemical interventions (such as anabolic
steroids) is to increase the individual’s capacity to train. In expressing this
uneasiness about biotechnical enhancement, we are not celebrating some fictitious
agency divorced from bodily events and consequences: whenever the body works or
is at work, the body’s underlying biology changes. Neither are we casting
doubts on efforts to improve the body by means that work on it directly; to do
so would require us to cast doubts on all of medicine and surgery, not to
mention a well-ordered diet. Yet on the plane of human experience and
understanding, there is a difference between changes in our bodies that
proceed through self-direction and those that do not, and between changes that
result from our putting our bodies to work and those that result from having
our bodies “worked on” by others or altered directly. This is a real
difference, one whose importance for the ethical analysis, as we shall see
later, may prove decisive.
Yet in trying to preserve the distinction between
intelligible agency and unintelligible agency—between getting better because of
“what we do” and getting better because of “what is done to us”—we face a
dilemma. Many of the basic activities of life—for example, eating, breathing,
and sleeping—transform our bodies without our directing the actual work of
transformation. Eating the right foods makes our system work better. Science
can come to understand why this is so—why protein is “good” and fats are “bad,”
or how our bodies break them down and to what effect. But these processes of
the body, however well understood, can never be made experientially
intelligible in the same way our self-directed activities are intelligible. We
digest and we dance, but digesting and dancing are very differently our
doings.
We can control the food we eat, but improving our native
digestion through practice is beyond our power. We dance by choice, both
immediately and self-consciously, with the movements of the body connected to
our active desire to dance and our self-awareness of dancing. Over time we can
see our dancing improve, at least within the limits of our native capacities,
and we can see that it is through our own practice that the superior performance
has occurred. Clearly, as with eating, what happens in our bodies as we become
better dancers is invisible and mysterious at the organic and molecular levels;
it is intelligible, if at all, only in the terms of science, not of human
experience. But the lived experience of dancing—of doing the deeds that enable
us to do them again and do them better—matters a great deal. When we dance, our
improvements are “our own,” made possible by and limited by our native biology,
but still the result of our own self-directed activity.
And here we begin to understand the complexity: To be a
human organism, possessed of a body all of whose activities are mediated by
invisible and molecular events, means that our identity is always to some
degree independent of all our self-conscious efforts to mold or control it. In
important ways, our bodily identity and our bodily capacities are inborn,
inherited, and “given,” and much of what our bodies do thereafter is shaped by
processes and in ways we do not direct or fully grasp at the level of inner
human experience. We cannot make our bodies into just anything we like, no
matter how hard we try. As human individuals, we are not simply the beings or
persons that we will ourselves to be, precisely because we are
biological beings—with finite capacities and a finite body, which make having
an identity possible in the first place. And yet, if there are limits to what
we can do, there are also possibilities. We can actively change our bodies and
change ourselves in important ways, precisely by trying, doing, working, and
performing the very activities we seek to do better.
Even in the most self-directed activities, we remain
ignorant, on the level of experience, of what is transpiring chemically in our
bodies. This fact has an important implication: The difference between
improving the body through training and improving it through diet or drugs is not
absolute but a matter of degree. Nevertheless, the fact that the difference
is one merely of degree does not make it humanly insignificant. Some acts are
more, and some acts are less “our own” as human and as individuals. When we
seek superior performance through better training, the way our body works
and our experience and understanding of our own body at work are more
closely aligned. With interventions that bypass human experience to work their
biological “magic” directly—from better nutrition to steroids to genetic muscle
enhancements—our silent bodily workings and our conscious agency are more
alienated from one another.
The central question becomes: Which biomedical
interventions for the sake of superior performance are consistent with (even
favorable to) our full flourishing as human beings, including our flourishing
as active, self-aware, self-directed agents? And, conversely, when is the
alienation of biological process from active experience dehumanizing,
compromising the lived humanity of our efforts and thus making our superior
performance in some way false—not simply our own, not fully human? Better
nutrition seems an obvious good, a way of improving our bodily functioning that
serves human flourishing without compromising the “personal” nature or
individual agency of what we do with our healthy, well-nourished bodies. But
moving outward from there, the puzzle gets more complicated. Where in the
progression of possible biological interventions do we lose in our humanity or
identity more than we gain in our “performance”? Is there a way to distinguish
coffee and caffeine pills to keep us awake from Modafinil to enable us to avoid
sleep entirely for several days, from amphetamines to keep us more alert and
focused, from human growth hormone, steroids, and EPO to improve strength and
endurance, from genetic modifications that make such biological interventions
more direct and more lasting? All of them alter our bodily workings; all of
them to varying degrees separate self-directed experience from underlying
biology.
Does that mean that we are incapable of distinguishing
among them, humanly and ethically? Can our disquiet about pharmacological and
genetic enhancement withstand rational scrutiny? More deeply, what does the
prospect of such interventions tell us about the nature of human activity and
the meaning of human identity? These are perhaps the deepest questions for the
ethical analysis that follows. But to see why this is so, we must first
consider some more familiar sources of ethical disquiet.
B.
Fairness and Equality
The most obvious disquiet with performance-enhancing agents
in athletics, both equipment like corked bats and biological interventions like
steroids, stimulants, or future genetic muscle boosters, concerns fairness: the
worry that players using them will have an unfair advantage over other players,
the concern that injustice will be perpetrated against one’s rivals. Games have
rules, and breaking the rules in these ways undermines the fairness of
competition and the dignity of the game. This is, of course, a proper concern.
But the question of fairness is more complicated than it looks at first.
Athletics, like many other human activities, depend on
native gifts that are unequally distributed. Indeed, human sport often
highlights and celebrates the very real differences and inequalities in our
biological “starting points.” In most sports, we do not, in the name of
equality, require that our athletes (or others) with special talents assume
handicaps so that everyone might compete on an equal footing.xvi
Although we may never settle the ancient and complicated question about how
much of our various achievements is due to “nature” and how much to “nurture,”
there is no question but that gifts of nature have much to do with all sorts of
human excellence. Many individuals, lacking certain physical and mental
attributes (for example, height, muscle potential, eye-hand coordination), will
never achieve the highest levels of human performance in certain activities no
matter how hard they strive. At the same time, nature is hardly the whole
story. Many individuals, with more limited native powers, will outperform those
who are less willing or less able to cultivate their superior gifts.
Some have argued that allowing performance-enhancing drugs
would be an acceptable—or even desirable—means of leveling a playing field that
is unequal by nature. It could make athletic competition more perfectly fair,
allowing winners to become those who do the best rather than those who are
the best. But others argue that such drugs would only exacerbate the naturally
unequal endowments rather than correct them. For even were there to be an “enhancement
commissar” who calculated what degree of “boost” each person needed in order to
get even with the natively gifted, there would be no way to titrate all the
relevant gifts.xvii
Besides, in a free country there would be no basis for denying the same
performance-enhancers also to the more talented. Why, if they wish it, should
those destined to be tall or bulky be refused a chance to become taller or
bulkier through growth hormone? As a result, those who are “best by nature”
would become even better by augmenting nature’s gifts with biological
enhancements. And whether we allow or disallow such enhancements, we are not
likely to alter the inherent biological inequalities that are part of being
human, and that are important for human excellence in sports and many other
activities. Fairness is always limited, to some degree, by the mysterious gifts
of nature, even if such gifts are not solely responsible or even decisive for
who will in the end become excellent or who will perform excellently.
The inequality of natural endowments highlights a related
dilemma regarding the standards of excellence: to what extent should we judge
performances superior for being “the best they can be,” rather than simply
being the “best”? For example, we celebrate both the real Olympics, which
measures the best of the best, and the Special Olympics, which measures the
best of those who strive in spite of great natural disadvantages. In the real
Olympics, we honor the best human runner, and we appreciate the fact that the
excellence of human running is not relative; it can be truthfully and quantitatively
measured. At the same time, we judge the Special Olympians according to a
different standard. We regard their activity as a kind of excellence—of
personal achievement rather than of absolutely superior performance—even as
they compete in the same activity with much lower scores. Standards of
excellence also change with the times. In some sports, the average professional
athlete of today probably has better scores and more physical strength than the
greatest champions of yesteryear. But which of these individuals—today’s
no-name or yesterday’s giant—do we judge as “superior” or more excellent?
In sum, there seems to be an “absolute” dimension to human
excellence: in certain activities, there is such a thing as the best human
performance. And yet, judging human excellence also depends on making sense of
nature’s unequal allotment of gifts, as well as the way particular human
activities, for various reasons, change over time. We need to fit our scales of
excellence to the thing being weighed, resisting the twin errors of believing
that all excellence is relative or that all excellence can simply be ranked and
determined by “score.”
Still, there is a danger of sentimentality, as well as of
confused thinking, in admiring athletes largely for the excellence of extra
effort. The perfectly fitting praise of the resolve, effort, and devotion
necessary to perform in the face of serious handicap is praise more for human
will and determination, less for superior performance as such. As we shall
emphasize below, human performance humanly done does involve human intention,
choice, and will; yet it would be strange to celebrate mainly human willfulness
in activities such as athletics that display, above all, bodily grace
and beauty. This observation suggests that, in athletics, it is the
harmonious and seemingly seamless fusion of mind and body that is crucial to
the athletic ideal of superior performance. Neither the human body regarded as
mere animal, nor the human body regarded as recalcitrant slave to be whipped
into shape by an unbending will, but the human being displaying in visibly
beautiful action the workings of heart, mind, and body united as inseparably as
the concave and the convex—that, as we shall argue shortly, is the heart of humanly
superior performance.
Finally, at least in sports, fairness understood as “playing
by the rules” is a matter of convention. When it comes to steroids, EPO, or
corked baseball bats, the concern about unfair advantage is to a large degree
self-created. It is only because these performance-enhancing agents are
disallowed, and because those who use them must do so outside the rules and
surreptitiously, that we regard their use as unfair. But if steroids were
declared legal in competition, everybody (or nearly everybody) who desired to
compete at the highest level in most sports might well use them. The problem of
fairness of access and extra advantage would largely disappear—though the
problem of natural inequality would remain. It is therefore not enough to
defend the rules (no steroids, no corked bats) and decry those who break them.
The rules themselves—why they exist and what they are defending—must be
understood and supported. This must be done on grounds that go beyond equality
and fairness toward others to the nature and meaning of the activity itself.
C. Coercion and Social Pressure
A second source of disquiet centers on issues of freedom
and coercion, both overt and subtle. The pride most nations (and schools) take
in their athletes is often far from benign, and there are well-known cases in
which countries and coaches have forced athletes to use performance-enhancing
drugs. In East Germany before the fall of communism, to take just a single
example, the young members of the women’s Olympic swim team took regular doses
of the anabolic steroid known as Oral-Turinabol. This improved their strength
and endurance, but it also caused terrible masculinizing side effects (severe
acne, uncontrollable libido, gruff voices, abnormal hair growth). Those women
who were brave enough to inquire about what they were taking were told that the
drugs were simply “vitamin tablets.” As one of the swimmers testified years
later: “I was fifteen years old when the pills started. . . . The training
motto at the pool was, ‘You eat the pills, or you die.’ It was forbidden to
refuse.”10
But the potential for coercion—or at least intense social
pressure—is certainly not limited to tyrannical regimes and despotic coaches.
Should the use of an enhancing agent become normal and widespread, anyone who
wished to excel in a given activity, from athletics to academics, might “need”
to use the same (or better) performance-enhancements in order to “keep up.”
Anecdotal evidence suggests that this “soft coercion” may already be a problem,
given the widespread underground use of illegal substances in many professional
sports. True, the individual users, in such circumstances, are still choosing
the drugs for themselves. They are free in a way the East German swimmers were
not. But their choice is constrained by the fact—or by the belief—that it would
be impossible to compete, or compete on an equal playing field, without them.
They see the alternative of not using them as a kind of “unilateral
disarmament,” virtually guaranteeing that only those individuals with every
biological advantage would excel or succeed. In professional sports, where not
only victory but big money is at stake, the pressures not to disarm oneself pharmacologically
will be—are already—enormous.
The point can be generalized beyond athletics, and when
this is done, we see additional reasons for concern. In a meritocratic and
results-oriented society such as ours, the vast numbers of people caught up in
the race “to get ahead” come to feel increasing pressures to enhance their
performance. Most are probably moved less by the desire for excellence, more by
the love of gain or the wish to beat out the next fellow. As mounting social
and economic competition keeps ratcheting up the pressures, people look for any
advantage that might win them the more lucrative or higher-status job or that
would increase their children’s chances of gaining admission to the more
prestigious schools. Under these social conditions, with spiraling love of gain
conjoined with rising demand for recognition, the temptation in all walks of
life to use biotechnologies for some “extra edge” probably rises with the
pressure to compete. Today, professional athletes—and those who dream of becoming
professional athletes—often succumb to the temptation. Tomorrow, the same might
be true in many other areas of human endeavor.
Yet these quite legitimate concerns about pressure and
constraint must be examined more closely. For the fact is that athletic (and
other) competition is, in important ways, constraining or pressure-filled by
nature. By becoming better, our opponents force us to match their improvements
or fall behind and fail. By the entirely accepted (and generally laudable)
means of training, dieting, or superior coaching, they challenge us to meet or
better their improvements. Moreover, the quest for excellence, even in
activities (like music or ballet) that are not in essence competitive,
typically comes with stiff demands, and anyone who is serious about superior
performance has little choice but to yield to or embrace them. The question
therefore becomes: Which demands and “necessities” of the pursuit of superior
performance are defensible and which are not? Which serve human excellence and
which compromise or undermine it?
Seen most clearly, the concern about coercion, as with
equality and fairness, turns out to be a pointer to other and deeper concerns,
concerns about what gives an individual performer his or her dignity, and what
makes an individual performance humanly excellent. If there is a core
difficulty here, it is with the biological enhancers themselves, not with the
fact that individuals might feel constrained or compelled to use them.
D. Adverse Side Effects: Health, Balance, and the Whole of Life
One of the central concerns about the biotechnical agents
themselves is the risk and reality of adverse and undesirable “side effects,”
in the first instance, on bodily health and safety. The unintended cost of
seeking stronger muscles and superior performance through drugs or genetic
engineering could well be bodily (or mental) harm. With drugs like steroids,
the grave long-term health risks are well known: they include, among others,
liver tumors, fluid retention, high blood pressure, infertility, premature
cessation of growth in adolescents, and psychological effects from excessive
mood swings to drug dependence. With looming biotechnical powers like genetic
muscle enhancement, the side effects are for now uncertain. But until proven
otherwise, it makes sense to follow this prudent maxim: No biological agent
powerful enough to achieve major changes in body or mind is likely to be
entirely safe or without side effects. Moreover, targeted interventions aimed
at enhancing normally functioning capacities, not repairing broken parts, could
produce lopsided “improvements” that throw whole systems out of kilter: monster
muscles could threaten unenhanced bones and ligaments.
The concern about safety is a real one: to be an athlete should
not mean accepting a sentence of premature death or serious disease or
disability, later if not sooner. As admirers of athletes, we should not want to
exploit those we most esteem; we should not want to use them up for our own
entertainment and satisfaction; and we should not want to treat our fellow
human beings as expendable animals. But the concern about safety must also be
subjected to scrutiny. Athletic activity is often intrinsically unsafe: Boxing
and football, hockey and skiing—such activities require daring, toughness, and
sometimes even contempt for “mere safety” as being far less important than
victory and achievement. Superior performances in these activities would be
less excellent or less genuine if fully stripped of their perils. Inasmuch as
risk and sacrifice are part of what it takes to be superior, one might even
argue that an athlete’s willingness to use such drugs, at so great a personal
cost, is not dehumanizing but admirable—a sacrifice of oneself to the game one
loves.
Of course, there seems to be a difference between the
uncertain dangers of the playing field and the deliberately self-inflicted harm
of using performance-enhancing drugs.Playing a game with the risk of great harm
seems different from inflicting high-tech, premeditated, long-term damage on
oneself to gain a short-term advantage. The hazards intrinsic to the game are
generally unavoidable, while those associated with taking the drugs are utterly
unnecessary. But again, we must wonder: Why should we value the long-term over
the short-term—the long healthy life over the short and glorious one? Isn’t
part of our admiration for athletics precisely the “gladiator spirit,”including
the willingness to forego “mere safety” for brief but memorablemoments on the
field of glory? Absent further analysis, there would seem to be a potential
nobility on the part of the athlete who seeks excellence at whateverpersonal
cost. And yet, there also seems to be something perverse, or ignoble, in coming
deliberately to abuse one’s body for the sake, presumably, of showing off its
beautiful and splendid gifts and activities. There seems to be something
dehumanizing in coming to rely so heavily on one’s chemist to excel, to the
point where one might wonder whether such excellence is still “personal” at
all.
Some enhancements, both here and coming, may become
physically safe, with few side effects that compromise the long-term health of
those who use them. Yet there are other consequences “to the side” that deserve
our concern, for such enhancements might change the body or mind in ways beyond
making them ill. For it stands to reason that drugs sufficiently capable of
affecting us in ways we desire are likely to affect us in ways that we do not
seek and cannot predict. Perhaps certain hormones that boost training capacity
and aggressiveness will make the individual emotionally less “well-balanced” in
everyday life. Or perhaps by taking drugs that increase tolerance for physical
pain, the individual will decrease his or her experience of other physical
pleasures. Part of the problem with certain biological enhancements, in other
words, may be that they isolate one set of human powers—the powers that make
for a superior runner, linebacker, or weight lifter—at the expense of other
areas of life: health, to be sure, but also calmness, balance, equanimity,
pleasure, creativity, and so forth. Such enhancements risk creating a distorted
form of human excellence—magnifying certain elements of human life while
shrinking others.
But the “distortions” of life in pursuit of superior
performance cannot be blamed on biotechnical enhancers alone. In any society in
which people feel driven by the desire for success, whether measured in terms
of wealth, power, or status, many human activities (including athletics) are
easily bent out of their natural shape in order to serve these external goals.
Yet the difficulty exists even when superior performance is pursued not for
outside ends but for its own sake. All human excellence, to some degree,
requires at least some distortion: putting aside many activities or aspirations
to excel in one; leaving several powers undeveloped to develop a few;
sacrificing most human goods to pursue a single one at the highest level; and
perhaps becoming so excellent in one particular area of human endeavor that
most other human beings only encounter such superior performance at a distance.
All excellence, in other words, requires at least some separation from the
majority: the separation required by long hours of practice and the separation
inherent in performing in the arena or on the stage. We need think only of the
strange life lived by Olympic gymnasts, often whisked away from normal
childhood at a very early age to enter the all-consuming world of the training
camp. Or the women’s Olympic volleyball teams that not only practice but live
in camp together 365 days a year for nearly the entire four years between the
quadrennial events. Sometimes this separation from others and from ordinary
life enables individuals to embody the best that human beings are capable of,
at least in a particular area of activity. At other times, the separation might
be so severe, and the way we pursue our chosen activity so distorting of the
human whole, that the dignity of the performer is called into question. He or
she might be a great athlete, but only by becoming inhuman in other ways.
Viewed more fully, the concern about side effects, beginning with health, gets
us to the deepest matters and the greatest “side effect” of all: that we
improve performance at the cost of our full humanity; that we become “better”
by no longer fully being ourselves.
E. The Dignity of Human Activity
The preceding analysis has considered several sources of
our disquiet about different technical and biotechnological agents that might
enhance or alter athletic performance: unfairness and inequality, coercion and
constraint, and adverse effects on the health and balance of human life. Each
has indicated something important; but none gets us to the core issue. The
problem is not simply inequality and unfairness, since our natural endowments
are unequal to begin with, and the conventions outlawing certain enhancements
could be changed to allow everyone equal access to the same technical and
biotechnological advantages. The problem is not simply coercive pressure, since
only if there is something intrinsically troubling about bioengineered
enhancements should we be really troubled by the pressures to use them,
especially given that “pressures” are inherent in the pursuit of athletic or any
other kind of excellence. And the problem is not simply health hazards and
adverse side effects, or the ways that enhancing certain human capacities might
limit or endanger other elements of human life. For the pursuit of athletic
(and other) excellences necessarily seeks something higher than mere safety,
and excellence nearly always requires putting aside some aspirations to pursue
others; the individual accepts less excellence in many aspects of life in order
to be excellent in this one. Yet the concern about compromising the whole of
life for the sake of one isolated part points us closer to the heart of the
matter: understanding the true dignity of excellent human activity, and how
some new ways of improving performance may distort or undermine it.
Our deepest concerns are tied to the large questions we
raised at the start of this chapter: What is a human performance, and
what is an excellent one? And what makes it excellent as a
human performance? For it seems that some performance-enhancing agents,
from stimulants to blood doping to genetic engineering of muscles, call into
question the dignity of the performance of those who use them. The
performance seems less real, less one’s own, less worthy of our admiration. Not
only do such enhancing agents distort or damage other dimensions of human
life—for example, by causing early death or sexual impotence—they also seem to
distort the athletic activity itself. It is not simply that our greatest
sportsmen could become bad fathers if their enhancements made them
uncontrollably aggressive or left them prematurely dead. It is that they are,
despite their higher scores and faster times, bad or diminished as sportsmen—not
simply because they cheated their opponents, but because they also cheated,
undermined, or corrupted themselves and the very athletic activity in which
they seem to excel.
What is at stake here is the very meaning of human agency,
the meaning of being at-work in the world, being at-work as myself,
and being at-work in a humanly excellent way. To clarify this
claim, we must consider several aspects of human activity and human agency.
Before doing so, we must first address the matter of competition and its
significance for the things we do.
1. The Meaning of Competition.
We have already noted, in the discussion of coercion and
constraint, the distortions that social pressures to get ahead introduce into
athletics and other human activities. Yet unlike many of our activities—such as
learning, doctoring, or even governing—athletics are intrinsically competitive.
They involve a contest of single opponents or opposing teams, matching their
talents against one another and seeking on that day or in this event to be
better than the rest (or better than the best). Sometimes competition is
friendly, a playful meeting of fellows who take pleasure in each other’s
achievements. Sometimes competition is fierce, mixed with a desire not only to
see oneself victorious but to see one’s opponent roundly defeated. Most often,
competition mixes the friendly and the fierce: good friends are often rivals on
the playing field, and bitter opponents often have a deep respect for one
another as being worthy foes, demanding and evincing one’s own best efforts.
But not all human activity, as we have noted, is
intrinsically competitive and rivalrous. Consider, as a comparison to human
sport, the activity of making music. It is certainly the case that musicians
sometimes compete with one another: for first chair in the orchestra, for
record contracts, for prizes and public esteem. But strictly speaking, when
engaged in these rivalries they are not at work making music. Indeed, it seems
misguided to say that music is in its essence a competitive activity—in
the way Olympic running and professional chess are intrinsically competitive
activities. When the string quartet or the symphony orchestra makes music, it
has no opponent against whom it is competing. Moreover, no musician’s
performance or excellence can be “measured” in the same way as the shot-putter’s
or the runner’s when he or she breaks a world record. To be sure, we can judge
some musical performances as clearly better than others, and individuals strive
to become better musicians than they were before. But the many forms of musical
excellence seem to belie final comparative judgments about better and worse:
two individuals can play the same sonata or sing the same song very differently
but both excellently, each capturing something essential but something
different in the music. Runners in the same race may run differently—with
different styles, each embodying a different form of excellent running—but in
the end we can say, at least in a given race, who is the “best.”
And yet, even those activities that are intrinsically
competitive, such as sports, are not simply competitive in their
essence. The dignity of athletic activity is not defined only by winners and
losers, faster and slower times, old records and new. Competition can sometimes
blind us to the fact that it is not simply the separable, measurable, and
comparative result that makes a performance excellent—but who is
performing and how. The word “superior” itself captures this dichotomy,
meaning both “better than one’s competitor” but also denoting a performance or
activity that is simply outstanding in itself. Excellent running seems to have
a meaning—the human body in action, the grace and rhythm of the moving human
form, the striving and exertion of the aspiring human runner—that is separable
from competition, even when the runner is running competitively. Even in the
most competitive activities, the deepest meaning may not be honorable victory,
or beating one’s best human opponents in a worthy way, but rather the human
agent at-work in the world—especially the lived experience, for both the
spectator and doer, of a humanly cultivated gift, excellently-at-work.
2. The Relationship between Doer and Deed.
This leads us to the second consideration: the relationship
between the doer and the deed, or between the human agent and the human
activities he or she engages in. As said above, the dignity of human sport (or
any other human activity) is determined not simply or predominantly by the
measured and separate result, but also by who achieves it and how.
Seen not as a detachable deed but as an activity of an agent, athletic
performance depends on both the doing of a deed and the identity
of the doer. The purpose of competitive running, for example, is to
cover the set distance as quickly as possible. But this is only part of the
story. The man on roller skates moves more quickly than the runner. But he
obviously engages in a different activity—moving quickly, but not running—and
thus should be judged according to a different standard. (Just because we have
invented roller skates, cars, and airplanes—all faster ways of moving—does not
mean we have stopped competing in running.)
Animals run, often quickly. In contrast with mechanized
movement, in animal running doer and deed are seamlessly united. And as already
noted, the average cheetah runs much faster than the fastest human being and is
beautiful to behold. But we do not honor the cheetah in the same way we honor
the Olympic runner, because the Olympian runs in a human way as a human
being. (Of this, more soon.) In a word, in athletic performance seen as a
performance of a performer, we cannot separate the “result” (the fastest time)
from the “activity” (human running). In assessing athletic performance, we do
not in fact separate what is done from how it is done and who
is doing it, from the fact that it is being done by a doer. And we
should not separate the score from the purpose of keeping score in the first
place: to honor and promote a given type of human excellence, whose meaning is
in the doing, not simply in the scored result. Tomorrow’s box score is
at most a ghostly shadow of today’s ballgame.
Consider another example: the best human chess player
playing against a chess-playing computer. It is worth asking how or whether man
and machine are really “competing” at all, and to what extent we can really
compare the superior capacity of a computer to “play” chess with the
distinctive excellence of a human chess player. On one level, of course, they
are indeed competing: playing the same game according to the same rules. And
yet, the computer “plays” the game rather differently—with no uncertainty, no
nervousness, no sweaty palms, no active mind, and, most importantly, with no
desire or aspiration and no hopes or expectations regarding possible future
success. In this new type of competition, our best human being faces off
against our best human artifact. But the computer’s way of “playing” is really
a kind of simulation—the product of genuine human achievement, to be sure,
since building such a computer is its own manifestation of human excellence.
But is this simulation the real thing—playing chess?xvii
And by building computers that “play” perfect chess, do we change the meaning
of the activity itself? Do we reorient the very character of our
aspiration—from becoming great human chess players to becoming better
chess-playing machines, or, if you prefer, from becoming great
chess players to producing the best-executed game of
chess? Why, if chess is no more than the sum of opposing moves that are in
principle calculable by a machine, would human beings wish to play chess at
all, especially if the machines can do it better?
The answer is at once simple and complex: We still play
chess because only we can play chess as human beings, as genuine
chess players. We still run because running, while not as fast as moving
on wheels, retains a dignity unique to itself and unique to those who engage in
this activity. The runner on steroids or with genetically enhanced muscles is
still, of course, a human being who runs. But the doer of the deed is,
arguably, less obviously himself and less obviously human than
his unaltered counterpart. He may be faster, but he may also be on the way to
becoming “more cheetah” than man, or more like the horses we breed for the
racetrack than a self-willing, self-directing, human agent. He does the deed
(running), and his resulting time may be measurably superior. But he is also
(or increasingly) the passive recipient of outside agents that are at least partly
responsible for his achievements.
3. Acts of Humans, Human Acts: Harmony of Mind and Body.
This brings us to a third and closely related
consideration, the specific difference of a human act or performance.
For in judging a performance to be genuinely and humanly superior, we care not
only that there be an integral connection between doer and excellent deed. We
care also that the doer-at-work display those qualities that make us admire the
performance as a human activity and as his own activity. Borrowing
a useful distinction from moral philosophy, not all acts done by humans
are human acts, acts that spring from the roots of our humanity. Not all
acts done by persons are personal acts.
One common way of getting at the crucial difference is to
talk about “true” and “false” acts, acts that do and acts that do not spring
truly from who or what we are. This is what people have in mind when they say
that athletes who use steroids or a corked bat to hit the ball farther than
they could before are not only breaking the rules, but getting their
achievements “on the cheap,” performing deeds that appear to be, but
that are not in truth, wholly their own. This makes sense as far as it
goes, but it gives rise to the question, “What would make an act of humans
genuinely a human act?” “What would make the deed truly one’s own?”
Comparison with the doings of animals other than man proves
helpful. In the activity of other animals, there is necessarily a unity between
doer and deed; acting impulsively and without reflection, an animal—unlike a
human being—cannot deliberately feign activity or separate its acts from itself
as their immediate source. Yet though a cheetah runs, it does not truly run a
race. Though it senses and pursues its prey, it does not seek a goal with full
consciousness or with ambitions to surpass previous performances. Though its
motion is voluntary (not externally compelled), it does not run by choice.
Though it moves in ordered sequence, it has not planned the course. Its beauty
and its excellence—and these are not to be disparaged—it owes largely to nature
and instinct.
In contrast, the human runner chooses to run a race and
sets before himself (herself) his (her) goal. He measures the course and
prepares himself precisely for it. He surveys his rivals and plots his
strategy. Though constrained by the limits of his flesh, he cultivates and
disciplines his body and its natural gifts in pursuit of his goal. The end, the
means, and the manner are all matters of conscious awareness and deliberate choice,
from start to finish. In a word, what makes the racer’s running a human act
humanly done is that it is done freely, knowingly, and by conscious choice.
So far so good. But if the humanity of our actions rests
solely on their being rooted in knowledge and conscious choice, we face this
difficulty: Is not a decision to enhance our bodies through drugs or genetic
intervention also a matter of human choice? Why would this not be precisely
the expression of our rational will, a manifestation of its peculiarly human
ability not to be enslaved by the limitations of our animal bodies? If it is
the presence of free, knowing, and conscious choice that makes for a human act,
then the bulking up of the genetically or drug-enhanced athlete—and
derivatively, his drug-assisted superior performance—would seem to be preeminently
human or even superhuman, a manifestation of our ability to transcend nature’s
and our personal limitations in a way no animal can.
This welcome objection invites a fuller account, with a three-part
response—one regarding the mind (and will), another regarding the body, the
third regarding their peculiar interrelations as expressed in athletics and
human activity more generally, as well as in human desire and aspiration.xix The
point about the mind has already been prepared by our earlier discussion of the
difference between gaining superior performance through training and practice
and gaining superior performance through biotechnological intervention and
engineering. We called attention to the difference between perfecting a
capacity by using it knowingly and repetitively and perfecting a capacity by
means that bear no relation to its use. And we stressed the difference, on
the plane of human experience and understanding, between changes to our
bodies that do and those that do not proceed through intelligible and
self-directed action, capable of being informed by the knowledge of human
experience. Thus, though the decision to take anabolic steroids to enhance
athletic performance can be said to be, in one sense of the term, a rational
choice, it is a choice to alter oneself by submitting oneself to means that are
unintelligible to one’s own self-understanding and entirely beyond one’s
control. In contrast with the choice to adopt a better training regimen, it is
a calculating act of will to bypass one’s own will and intelligibility
altogether.
Yet the problem with biotechnical enhancement lies not
merely on the side of exaggerated and self-contradictory willfulness. It lies
also with its mistaken identification of the human with the merely rational and
its neglect of our embodiment. For the humanity of athletic performance resides
not only in the chosenness and intelligibility of the deed. It depends
decisively on the performance of a well-tuned and well-working body. The body
in question is a living body, not a mere machine; not just any animal body but
a human one; not someone else’s body but one’s own. Each of us is personally
embodied. Each of us lives with and because of certain bodily gifts that owe
nothing to our rational will. Each of us not only has a body; each of us also is
a body.
In few activities is this truth more manifest than in
sports. When we see the outstanding athlete in action, we do not see—as we do
in horse racing—a rational agent riding or whipping a separate animal body.
What we mainly see is a body gracefully and harmoniously at work, but at work
with discipline and focus, and tacitly obeying the rules and requirements of
the game. We can tell immediately that the human runner is engaged in
deliberate and goal-directed activity, that he is not running in flight moved
by fear or in pursuit moved by hunger. Yet while the peculiarly human character
of the running is at once obvious, the “mindedness” of the bodily activity is
tacit and unobtrusive. So attuned is the body, and so harmonious is it with
heart and mind, that—in the best instance—the whole activity of the athlete
appears effortlessly to flow from a unified and undivided being.xx
At such moments the athlete experiences and displays
something like the unity of doer and deed one observes in other animals, but
for humans that unity is a notable achievement which far transcends what
mere animals are capable of. A great sprinter may run like a gazelle, a great
boxer may fight like a tiger, but one would never mistake their harmony of body
and soul for the brute instinct that spurs an animal toward flight or fight.
Athletic activity is not only generically human and
manifestly a bodily matter; it is also emphatically the work of particular
individuals. This is hardly accidental. Although we are all equally embodied,
we are not bodily identical. On the contrary, our differing identities are
advertised and displayed in our unique bodily appearance. True, in many gifts
of body and mind we are indistinguishable from our fellow human beings; but in some
gifts many of us are specially favored. It is the special distribution and
assortment of common and particular gifts, allotted to each of us, that
constitute the biological beginnings of our individual identity. In pursuing
superior athletic (or other) performance, we are cultivating and exercising
both our common and our particular gifts, seeking our own individual
flourishing. We discipline our gifts through choice and effort in the service
of enabling them to shine forth in our own beautiful and splendid activity. We
take pleasure in our own performance and achievement. The added bonus of
victory and the recognition that follows from it we esteem largely because they
confirm that our own embodied excellence has been attained and that our desire
for superior performance has been satisfied.
In trying to achieve better bodies through muscle-enhancing
agents, pharmacological or genetic, we are not in fact honoring our bodies or
cultivating our individual gifts. We are instead, whether we realize it or not,
voting with our syringes to have a different body, with different native
capacities and powers.xxi
We are giving ourselves new and foreign gifts, not nature’s and not our own,
and—exaggerating, but in the direction of the truth—treating ourselves rather
as if we were batting machines to be perfected or as superior horses bred for
the race and bound to do our bidding. These acts of will do not respect either
our own individuality or the dignity of our own embodiment—on which, by the
way, our will absolutely depends for its very existence.
At the root of all human activity is desire or aspiration,
especially when it aims at excellence. Human aspiration for superior performance,
for excellent activity, for something memorable and great, is not, finally, the
product of pure reason or pure will. Neither is it merely the product of our
animality. It stems rather from that peculiar blending of mind and desire,
perhaps peculiar to human beings, called by the Greeks eros, the longing
for wholeness, perfection, and something transcendent. In one formulation, it
is the desire: (1) for the good, (2) to be one’s own, (3) always.11
The root of this longing lies in the awareness that, alas, we are not entirely
unified and undivided beings. We are rather frail and finite in body and
conflicted in soul. Being conscious of our finitude and self-division, we
strive to make of ourselves something less imperfect, something more noble,
something fine—something that would be fulfilling as much as is humanly
possible. Further, we pursue this aspiration as ourselves and—at least to begin
with—for ourselves. We would not seek excellence on condition that, in order to
attain it, we would gladly have to become someone or something else.xxii
Not the excellence of god or beast, not even the excellence of some generic
human person or disembodied human will, but the excellence of our own embodied
allotment of human possibility is our goal. It is doubtful, to say the least,
that biotechnical transformations of our bodies—or minds—will contribute to our
realizing this goal for ourselves.
The ironies of biotechnological enhancement of athletic
performance should now be painfully clear. First, by turning to biological
agents to transform ourselves in the image we choose and will, we in fact
compromise our choosing and willing identity itself, since we are choosing to
become less than normally the source or the shapers of our own identity. We
take a pill or insert a gene that makes us into something we desire, yet only
by seeming to compromise the self-directed path toward its attainment. Second,
by using these agents to transform our bodies for the sake of better bodily
performance, we mock the very excellence of our own individual embodiment that
superior performance is meant to display. Finally, by using these technological
means to transcend the limits of our natures, we are deforming also the
character of human desire and aspiration, settling for externally gauged
achievements that are less and less the fruits of our own individual striving
and cultivated finite gifts.
There is, we might add, no limit in principle to the desire
to transcend the limits of our own nature. The desire to have a perfect body,
one that perfectly executes the dictates of the will, is tantamount to a desire
to transcend our embodiment altogether, to become as gods, to become something
more-than-human. No doubt the longing for perfection has inspired many of the
greatest human achievements. But unless guided by some idea of the character of
human perfection, such longings risk becoming a full-scale revolt
against our humanity altogether. Fueled in addition by a thirst not merely to
excel but to defeat and surpass our rivals, the desire for superhuman powers
easily becomes boundless.
The argument we have offered seems to have landed us in
this strange position: We seek to defend human willing or agency, in the sense
of defending our being what we really do. But we also seek to recognize the
biological limits of the will, in the sense that much that is central about us
is not truly our doing. Biotechnology seems to promise the triumph of the will
with less willing effort and bodily excellence in bodies not quite ours: we can
become what we desire without being the responsible and embodied agents of our
own becoming. A more human course, however, might be accepting that we cannot
will ourselves into anything we like, but we can still live with the dignity of
being willing, self-directed, embodied, and aspiring persons, not biological
artifacts, not thoroughbreds or pitching machines. Better, in other words, to
be great human runners with permanent limitations than (non)human artifacts
bred to break records.
Though our subject has not been athletics as such, but the
uses of biotechnical means to enhance athletic performance, our analysis casts
light on the ways in which the currently popular view of sports may already be
corrupting genuine human excellence and may lead, unless we change our tastes,
to enormous pressure to pursue any and all biological performance-enhancers,
should they be safe and effective. For we have long since blurred the line
between athletics and entertainment. If the baseball-loving public cares mainly
about how many homers are hit or how far they go, then it will matter less how
much the deeds flow from the unadulterated yet cultivated gifts of the hitter.
Only if superiority of performance continues to mean not just the excellence of
a detached act, but of the act as displaying the excellence of a superior human
being, excellently at-work—in our own mindful and aspiring embodiments—can we
preserve the full sense of humanly superior performance.
F. Superior Performance and the Good Society
Much of the above analysis focuses on the excellence of the
individual person at-work in the world. But any analysis of superior
performance must also take into account the performer’s relationship with
others: teammates and competitors, teachers and admirers, co-workers and
friends, as well as the larger community. It is true that the individual, even when
working in tandem with his fellows, is excellent as himself. But excellent
human activity is by nature situated within a community, a society, and a
culture. The human individual flourishes as himself, but he does not flourish
alone. And he rarely flourishes without enormous contributions from others,
people near and even far to whom he is indebted for nurture, rearing, coaching,
encouragement, employment, and the appreciation and support of the activity in
which he gets the opportunity to excel. Likewise, all excellence is particular
to time and place, even if particular examples of human excellence are “for all
time,” and even if we can admire those who perform in activities that we no
longer engage in ourselves.
In myriad ways, society has a stake in excellent human
activity. It rewards, honors, and nourishes the superior performances of its
members. But it also expects, demands, and depends upon them. In many everyday
functions—flying airplanes, fixing computers, educating children—we rely on others
to “get the job done” or “rise to the occasion” when needed. We need them to
perform and perform well, not just occasionally or sporadically, but steadily
and reliably. Allowing some leeway to beginners, we expect practice will make
perfect, we expect people to improve on the job and through the experience of
repeated performance.
Beyond its everyday utility, superior performance also ennobles
society: it makes everyone better; it raises the spirits of a community; it
nourishes the desire to be better and to do better, as individuals and as a
people. The example of superior performers gives those who are still developing
an image of who or what they might aspire to become themselves. And everyone
may be elevated by discovering that human beings—like them in being human,
unlike them in the superior ways they perform—can do the beautiful and
marvelous things they themselves cannot do, but in which they can surely, if
only partially, participate as appreciators and admirers.
Our analysis of human sport sheds light also on the entire
range of such socially valuable and excellent performances, both those that
adorn our community and those that make it possible. Each of these human
activities has its own character and meaning, and hence also its own dignity. In
music, as in sport, the body is gracefully at work, but at work in a different
way: the fingers striking the keys, the hand and arm moving the bow, the voice
singing at perfect pitch. The musician takes inspiration from others—perhaps
including rivals—but he does not compete. He makes music—arranging notes
and melodies as a composer and playing them as a performer. But he also captures
what is musical—hitting notes and singing harmonies as they were meant to be
hit and be sung. He knows the notes and his body knows the movements. And
guiding it all is his musical understanding of the musical whole, grasped in
both heart and mind, that both inspires the performance and that is, when given
life in the playing, its completion.
In a similar way, one might describe a range of other human
activities—painting, dancing, building, designing, writing. Each of these
activities has a distinct character and excellence, and each retains a dignity
unique to itself, demanding and rewarding different human powers and capacities.
But each of them, like sport, involves a humanly cultivated gift, a human doer
and human deed, a deed performed, at its best, in a humanly excellent way. It
is the human musician, not the synthesizing machine, whom we admire and
defend: the musician with desire and fallibility, who creates what did not
exist before and rises to the occasion when the moment most demands it. Most
important, while such superior performances are the work of individuals, all of
society shares in their excellence, as it always does when taste is receptive
to genius. Properly appreciative witnessing is participating, and it
enables everyone present to experience the surpassing human possibility in a
passing human moment.
In addition, even those activities necessary for life in
society and devoted to some external result or purpose—for example, human work
to produce some useful object or to perform some needed service—can be done in
a way that is dignified or undignified, human or dehumanizing. The difference
is not simply how many objects are produced, with what efficiency and what
effectiveness. What matters is that we produce the given result—the objects
that we make—in a human way as human beings, not simply as inputs who produce
outputs. Indeed, it is here that the temptation to improve performance—to make
workers more focused by giving them Ritalin, less sleepy by giving them
Modafinil, more muscular by genetically enhancing their muscles, and so on—is
most tempting. If all that matters is getting more out of them—or more out of
ourselves, by any means possible—then improving performance by every
biotechnical intervention available makes perfect sense. But as we have seen
with human sport, more is at stake than simply improving output. What matters
is that we do our work and treat our fellow workers in ways that honor all of
us as agents and makers, demanding our own best possible performance, to be
sure, but our best performance as human beings, not animals or machines.
But there is one further complication. Defending what is
humanly good or excellent must not only guard against the possibility of
dehumanization; it must defend first against the many threats to personal or
communal survival itself. When the very existence of the human agent or human
society is at stake, certain special superior performances are not only
edifying but urgent: for example, the superior performance of soldiers or
doctors. What guidance, if any, does our analysis provide for such moments of
extreme peril and consequence, in war or in medicine, when superior performance
is a matter of life or death? Are some biotechnical interventions to enhance
performance justified in these activities (surgery, war) while not justified in
the other activities of human life (sports, music, test-taking)? In these
circumstances, might we treat men as alterable artifacts—or willingly become
artifacts ourselves—in order to “get the job done”?xxiii
There may indeed be times when we must override certain
limits or prohibitions that make sense in other contexts—offering steroids to
improve the strength of soldiers while rejecting them for athletes, offering
amphetamines to improve the alertness of fighter-pilots while rejecting them
for students, offering anti-anxiety agents to steady the hands of surgeons
while rejecting them for musicians. When we override our own boundaries, we do
so or should do so for the sake of the whole, and only when the whole itself is
at stake, when everything human and humanly dignified might be lost. And we
should do so only uneasily, overriding boundaries rather than abandoning
them, and respecting certain ultimate limits to ensure that men remain human
even in moments of great crisis. For example: Even if they existed, and even in
times of great peril, we might resist drugs that eliminate completely the fear
or inhibition of our soldiers, turning them into “killing machines” (or “dying
machines”), without trembling or remorse. Such biotechnical interventions might
improve performance in a just cause, but only at the cost of making men no
different from the weapons they employ.
This particular case, in short, is the exception that
proves the rule: even in moments of great crisis, when superior performance is
most necessary, we must never lose sight of the human agency that gives
superior performance its dignity. We must live, or try to live, as true men and
women, accepting our finite limits, cultivating our given gifts, and performing
in ways that are humanly excellent. To do otherwise is to achieve our most
desired results at the ultimate cost: getting what we seek or think we seek by
no longer being ourselves.
We are well aware that this assessment of human activity
and human dignity, highly philosophical, may not be persuasive to some people.
And even those who might share the foregoing views of the possible corruptions
of using direct biotechnical intervention to gain superior performance might be
reluctant to argue against it for others. In a free country, so they might say,
people should be allowed to take their muscle enhancers or alertness pills,
even if we would not use them ourselves. Where’s the harm if some football
players here and there take steroids or a few ambitious college-bound students
take stimulants before their SATs?
Perhaps none. Human life is complicated, innovations
abound, and human activities often change their character without necessarily
losing their integrity. But we must at least try to imagine what kind of
society we might become if such biotechnical interventions were to become more
significant in their effects and more widespread in their use. We might come to
see human running and dog races, singers and synthesizers, craftsmen and
robots, as little different from one another. Human beings, here mostly for our
entertainment or our use, might become little more than props or prop-makers.
We might lose sight of the difference between real and false excellence, and
eventually not care. And in the process, the very ends we desire might become
divorced from any idea of what is humanly superior, and therefore humanly worth
seeking or admiring. We would become a society of spectators, and our
activities a mere spectacle. Or a society of parasites, needing and taking, but
never doing or acting. Worst of all, we would be in danger of turning our
would-be heroes into slaves, persons who exist only to entertain us and meet
our standards and whose freedom to pursue human excellence has been shackled by
the need to perform—and conform—for our amusement and applause.
For a while—perhaps indefinitely—we might relish the
superior results that only our biotechnical ingenuity made possible: broken
records on the playing fields, more efficient workplaces, improved national SAT
scores. But we would have gone very far, potentially, in losing sight of why
excellence is worth seeking at all, and hence what excellence really is, and
how we pursue it as human beings, not as artifacts.
Footnotes
i. This chapter is, accordingly, about both the excellence and
the humanity of “superior performance,” and about whether improvements in
performance do or do not compromise the humanity or individuality of the agent.
ii. Other areas where this is also true include music, dance,
theater, and other performing arts.
iii. Similarly, the things that can corrupt, tarnish, or merely
complicate sports—greed, vanity, the desire to injure or crush a rival—can
corrupt, tarnish, or merely complicate most other human activities.
iv. We leave out of the account some further enhancements of “running,”
such as the use of wheels, or even motors, on the soles of shoes. Such changes,
of course, would transform the activity into something other than running.
v.The age-related loss of muscle size and strength has been named “sarcopenia.”
(The term “sarcopenia” was first suggested by I. H. Rosenberg in 1989. It is
derived from Greek words meaning “poverty of flesh.” See Rosenberg, I., “Summary
Comments,” American Journal of Clinical Nutrition 50: 1231-1233, 1989.)
We shall consider sarcopenia further in Chapter Four, “Ageless Bodies.”
vi. The very idea of “muscle-bound” looks away from activity, and
implies restricted freedom of motion; the hypertrophied muscles cut down
somewhat the range of possible motion around some joints.
vii. Interestingly, female bodybuilders initially pursued the
same path as the males. The result was women bodybuilding champions with
smaller but similarly individually developed and articulated skeletal muscles.
More recently there has been an aesthetic reaction against the resulting female
muscle “overdevelopment” and, commercially at least, the more popular and
profitable activity today is women’s fitness competition.
viii. Recombinant viruses, engineered to express a specific foreign
gene, are frequently used to stimulate the production of functionally effective
amounts of the foreign protein to treat disease. Recombinant viruses created
from genetically engineered human Adenovirus-associated Virus (AAV) have proved
to be efficient delivery systems of foreign genes into muscle cells. As AAV is
a small virus, only small foreign genes can be used effectively with this
virus. Fortunately, the DNA sequence encoding IGF-1 is small enough to function
well in AAV-based recombinant viruses.
ix Professor H. Lee Sweeney, the leader of the team conducting
this research, gave a fuller description of his group’s recent findings in his
presentation to the Council in September 2002. According to Professor Sweeney,
the insertion of IGF-1 genes into mouse muscles not only blocked the normal
age-related decline of muscle size and strength; in addition, the researchers
found, it caused the muscle tissue of older mice to retain the optimal power
and speed normally found only in younger mice. It also improved the rate of
repair of damaged muscle tissue. Other experiments on rats showed that, when
IGF-1 gene injections were accompanied by strenuous exercise, not only did the
rats develop bigger and stronger muscles, they also retained those enhanced
muscles far longer than they normally would after the exercise had ceased.
Should comparable results be attainable with human skeletal muscles, gene
insertion would appear to hold great promise, both as therapy for muscular
dystrophy and age-related sarcopenia and as a means to enhance athletic
performance. See Sweeney, H., “Genetic Enhancement of Muscles,” presentation at
the September 2002 meeting of the President’s Council on Bioethics, Washington,
D.C. Transcript available on the Council’s website, www.bioethics.gov.
x. (From previous page.) In this study, approximately 1010
recombinant AAV particles in 100 microliters of fluid were injected into a
single small muscle compartment of mice. If such treatments were eventually to
be applied to humans, large amounts of recombinant AAV containing the human
IGF-1 DNA sequence would be required. Assuming such future treatments were
shown to be safe and effective, producing sufficient recombinant AAV to treat
millions of dystrophic and aging humans would remain a substantial logistical
challenge. However, there may be ways around this logistical problem involving
the production and transplantation of human muscle stem cells engineered to
produce more IGF-1.
xi. The growing understanding of muscle physiology at the
molecular level coupled with sophisticated genetic engineering has made it
possible to enlarge skeletal muscles selectively, without damaging heart
muscles in the process. In previous studies of this type, the IGF-1 transgene
was not connected to gene expression regulatory elements that restricted
production of mIGF-1 to muscle tissue. This led to overproduction of IGF-1 in
the circulation, and eventually to pathological enlargement of the heart
muscle. But in the studies with transgenic mice cited here, the rat mIGF-1
transgene was connected to gene expression regulatory elements that restricted
production of the rat mIGF-1 protein only to muscle tissues containing
primarily fast-twitch fibers. Side effects on the heart muscle did not occur.
xii. The first approach would be similar to other human gene
therapy projects in children and adults. The appropriately regulated human
mIGF-1 gene would be combined with a vector capable of efficient delivery to
muscle cells, perhaps AAV. This material could be produced in large volumes,
carefully characterized by tests in experimental animals, stored frozen and
used as needed. While the logistics of producing the large amounts of
recombinant AAV that would be required for treatment of thousands or millions
of patients are daunting, in principle this would be possible. The advantages
of this approach are (1) that it would develop and use a single,
well-characterized biological agent; (2) that treatment could be started very
slowly by introducing the recombinant mIGF-1 gene-containing AAV into one
muscle at a time and evaluating its effects; (3) that treatment could be
stopped immediately if untoward side effects developed. Disadvantages include
(1) the possibility that a large number of injections would be necessary to
treat each of the large number of human skeletal muscles; (2) the possibility
that this would not be an effective treatment for humans who had antibodies to
AAV as a consequence of a previous infection.
The second approach is a radical proposal, as it envisions treatment of
blastocyst-stage human embryos in vitro with a genetic procedure that was
intended to change the early development of skeletal muscle size and strength
and reduce the rate of loss later in life. This approach shares some advantages
with the first approach in that (1) a single biological agent could be prepared
and characterized that could treat all embryos; (2) only a single treatment
early in embryonic development would be needed, instead of multiple injections
into different muscles. The major disadvantages of this approach are the
difficult ethical questions it would raise, as well as the difficulty of
meeting the safety criteria demanded of any germ-line or embryo genetic
engineering (see Chapter Two, “Better Children”).
The third approach depends upon the ability to isolate human muscle stem
(satellite) cells and expand them in vitro. [This has recently been reported
for mice. See Qu-Peterson, Z., et al., “Identification of a novel population of
muscle stem cells in mice: potential for muscle regeneration,” Journal of
Cell Biology 157(5): 851-864, 2002.] The isolated human muscle stem cells
would then have their mIGF-1 production genetically modified by introducing an
appropriately regulated exogenous mIGF-1 gene copy. In theory, this could
produce modified muscle stem cells that multiplied continuously in vitro to
produce larger numbers of cells, and that differentiated appropriately in
vitro. In this case, genetically modified satellite cells would be injected
into skeletal muscles. The advantages of this approach include (1) it would
develop and use a single, well-characterized biological agent to modify the
muscle stem cells in vitro, and (2) the dose of modified stem cells could be
varied as necessary to optimize treatment of individual skeletal muscles. The
disadvantages include the possibility that a separate preparation of muscle
stem cells would have to be made from each patient needing treatment, in order
to get around the immune-rejection problem.
xiii. Earlier this year, the FDA enlarged the domain of approved
uses for human growth hormone to include preventive treatment of short stature.
To be eligible for approved use, a child’s height must be more than 2.25
standard deviations below the mean for age and sex; that is, he or she must be
among the shortest 1.2 percent of children. Obviously, successful treatment of
this group would automatically create another group of children who were now
the shortest 1.2 percent. Even before there was FDA approval, the uses of
growth hormone were already expanding, with increasing acceptance of medical
intervention for social gains. In an August 1996 article in the Journal of
the American Medical Association, Leone Cuttler and colleagues report that
six out of ten children receiving growth hormone are not actually
growth-hormone deficient. Some of these children have other medical problems
that stunt growth, but many receive treatment because their parents simply want
their children to be taller. (Cuttler, L., et al., “Short stature and growth
hormone therapy: a national study of physician recommendation patterns,” Journal
of the American Medical Association 276: 531-537, 1996.)
xiv. It has been suggested that along with the regular Olympics
and the Special Olympics, we have the “Bio-Olympics,” where the competition is
unconstrained and the athletes are free to use any legal form of pharmaceutical
or physiological enhancement.
xv. Better equipment is thought to be better because it does
what old equipment did more effectively. But as it does so, the activities in
which the old equipment was used are also altered, and not necessarily improved
as a whole. We certainly have better tennis rackets—but is the game
better now than it was then? We certainly have better weapons—but are the
soldiers of today humanly superior to the soldiers of old, and is warfare today
“better” than it used to be?
xvi. This bizarre prospect, the logical extension of a
preoccupation with equality, is the ingenious conceit of a short story by Kurt
Vonnegut, “Harrison Bergeron,” in his collection, Welcome to the Monkey
House. The goal is accomplished by the work of a “handicapper general” who
is charged with weighing down all elevated gifts, physical and mental.
xvii. Even beyond the native gifts, we could never titrate the
important advantages of proper nurture, rearing, coaching, encouragement,
experience, or faith.
xviii. Would anyone be interested in watching a chess match “played”
by two computers? If so, why? Would that be a “chess match” in any
ordinary sense?
xix. These questions about mind, body, and their interrelation, we
are well aware, are deep and difficult philosophical matters. We have no
illusion that we have done more here than signal their crucial importance to
the ethical analysis at hand.
xx. The perceived “at-one-ness” of the runner can produce a
parallel sense of at-one-ness in the spectators, also manifesting mind, body,
and heart. Unselfconsciously we spectators are stunned by the manifestation of
genuine human excellence: it holds our attention, it takes away our breath; it
wins our heart. In appreciating seamless excellence, we have moments of
seamless excellence ourselves, sharing reflectively in the glory of the
superior human performance we are witnessing. This “superior performance” of
the spectators has important implications for the character of the whole
society, a matter to which we return in the final section of this chapter.
xxi. To be sure, these transforming agents do not in fact produce
a completely different body. And a steroid-enhanced athlete probably still
feels that he is the same person he was before the treatment. But the fans,
seeing him for the first time in his new physique, so suddenly acquired, often
wonder if the newly minted slugger really has the same body, really is the “same”
person. More important, the implicit aspiration, even in these modest
transformations, is indeed to have a body more perfect than one could ever
acquire simply by cultivating one’s own natural gifts. In this sense, using
these agents on one’s muscles expresses the same desire as having major
cosmetic surgery on one’s face: to become, to some extent, someone else,
someone with a more perfect body. The use of analogous agents on one’s
psyche—say, to acquire a superior temperament or a different set of memories—is
likewise a (tacit) aspiration to become someone else. We shall explore this
subject in Chapter Five, “Happy Souls.”
xxii. For example: No sane person, we suggest, would choose to be
the fastest runner on two legs if it required becoming an ostrich. And few
people would choose to acquire someone else’s perfections of body or mind on
condition of becoming that other person. Who, in the event of such
self-transformative improvements, would we say now enjoyed them?
xxiii. Though both are concerned with matters of life and death,
soldiering and doctoring are different. The two “wholes” that they serve are
different, the community being both more comprehensive and much less
intrinsically perishable. The existence of all individual life within a
community depends on the survival of that community. An argument could be made
to cut soldiers a bit more slack than physicians in doing whatever it takes to “get
the job done,” precisely because the whole itself is at stake in time of war. A
counter-argument could also be made, not on the basis of the superiority of the
good being served, but rather the means used (cutting the body to heal it
versus cutting the body to kill it), which might justify cutting more slack to
surgeons than to soldiers.
_________________
Endnotes
1. Tzankoff, S., “Effect of Muscle Mass on Age-Related BMR
Changes,” Journal of Applied Physiology 43: 1001-1006, 1977.
2. Asakura, A., et al., “Muscle satellite cells are
multipotential stem cells that exhibit myogenic, osteogenic, and adipogenic
differentiation,” Differentiation 68(4-5): 245-253, 2001; Zammit, P., et
al., “The skeletal muscle satellite cell: stem cell or son of stem cell?” Differentiation
68(4-5): 193-204, 2001.
3. This discussion owes much to the work of Professor H. Lee
Sweeney and his colleagues at the University of Pennsylvania and elsewhere (see
Bibliography), and to his description and discussion of that work at the
September 2002 meeting of the President’s Council on Bioethics. Transcript
available at the Council’s website, www.bioethics.gov.
4. Barton-Davis, E., et al., “Viral mediated expression of
insulin-like growth factor I blocks the aging-related loss of skeletal muscle
function,” Proceedings of the National Academy of Sciences 95:
15603-15607, 1998.
5. Musaro, A., et al., “Localized Igf-1 transgene expression
sustains enlargement and regeneration in senescent skeletal muscle,” Nature
Genetics 27: 195-200, 2001.
6. H. Lee Sweeney, personal communication with Council staff,
2002.
7. Weber, M., “Effects of growth hormone on skeletal muscle,” Hormone
Research 58(3):43-48, 2002.
8. Gladwell, M., “The Sporting Scene: Drugstore Athlete,” The
New Yorker, September 10, 2001.
9. Rousseau, “Discourse on the Origin and Foundations of
Inequality (Second Discourse),” transl. Roger D. and Judith R. Masters, in The
First and Second Discourses, ed. Roger D. Masters, New York: St. Martin’s
Press, 1964, p. 147.
==============================
Chapter
4. Ageless Bodies
Try as we might to improve or enhance our performance, we
all know that it is bound to degrade over time. As the body ages, its abilities
decline: we lose strength and speed, flexibility and reaction time, mental and
physical agility, memory and recall, immune response, and overall functioning.
We know that in the end, and generally as a result of this accumulation of
debilities, our bodies will give out, and our lives will end.
The inevitability of aging, and with it the specter of
dying, has always haunted human life; and the desire to overcome age, and even
to defy death, has long been a human dream. The oldest stories of many
civilizations include myths of long lives: of ancients who lived for hundreds
of years, of faraway places where even now the barriers of age are broken, or
of magical formulas, concoctions, or fountains of youth. And for several
centuries now the goal of conquering aging has not been confined to magic and
myth; it was central to the aspirations of the founders of modern science, who
sought through their project the possibility of mastering nature for the relief
of the human condition—decay and death emphatically included. But it is only recently
that biotechnology has begun to show real progress toward meeting these goals,
and bringing us face to face with the possibility of extended youth and
substantially prolonged lives. Using rapidly growing new knowledge about how
and why we age, scientists have achieved some success in prolonging lifespans
in several animal species. To be sure, there is at present no medical
intervention that slows, stops, or reverses human aging, and for none of
the currently marketed agents said to increase human longevity is there any
hard scientific evidence to support the hyped-up claims.1
Yet the prospect of possible future success along these lines raises high
hopes, as well as profound and complicated questions.
To elucidate these hopes, and to introduce these questions,
we will examine some of the potential techniques for the extension of longevity
and youthfulness, and some of their imaginable consequences. Our aim here, as
throughout this report, is not primarily to analyze the details of the
scientific prospects, or to predict which techniques might prove most effective
in retarding aging. Rather we consider a range of reasonably plausible
possibilities in order to discern their potential human and ethical
implications.i
But before we can begin to examine such possibilities, we must inquire about
the underlying desire. What do we wish for when we yearn for “ageless bodies”?
I. The Meaning
Of “Ageless Bodies”
It may at first seem strange to suggest that we yearn for
an “ageless body,” not a term commonly heard and certainly not the conscious
and explicit longing of very many people. Still, when properly examined,
something like a desire for an “ageless body” seems in fact to be commonplace
and deeply held; and should our capacities to retard the senescence of our
bodies increase, that desire may well become more explicit and strong.
We all know at least something of what it is to age, but
perhaps we have not often enough given thought to the full place of aging in
human experience, and to the significance of the nearly universal desire to
defy or to stop it. We measure our age in terms of years we have lived, and in
that sense there is no stopping aging. Time marches on incessantly, and we are
ever dragged along right with it. But we experience aging not just as the
passage of time, but rather also as the effect of that passage on us: on our
bodies, our minds, our souls, and our lives. In this respect, aging has two
contradictory faces. Generally speaking, our physical and mental faculties
degrade as we age, but often our understanding and judgment can improve. Our
bodies grow frail under the weight of the years, but our wisdom—we hope—may
grow greater as our store of experience swells.
It is only the former of these facets of aging that we
rebel against and seek to push away. We want still to grow wiser or at least
less foolish with age, but we wish we could do it without growing weaker. We
mean not so much to slow the passing of the years as merely to shield our
bodies from brutal bombardment by the silent artillery of time (in Abraham
Lincoln’s memorable phrase). That way, we might be in a position to make more
practical use of our hard-earned wisdom, and youth would not be so carelessly
wasted on the young. As C.S. Lewis put it: “I envy youth its stomach, not its
heart.”
In this sense, it is fundamentally the aging of the body
we wish to stop. Indeed, we experience bodily decline as in many respects a
kind of betrayal, as our body, once youthful and vibrant, seems somehow less
responsive to our will, and less capable of executing some once routine demands
of daily life. We wonder, together with Shakespeare, “is it not strange that
desire should so many years outlive performance?”2
And this betrayal grows worse with time, and step by step we find ourselves
less able and competent in many of life’s activities. We feel keenly what we
have irreversibly lost, and worse yet, we know that much of the strength that
remains will also be lost over time.
But it is more than the dread of decline that motivates us
to seek ageless bodies. The corruption of the body brought on by aging points
necessarily in the direction of eventual death, and unexpected encounters with
new and unfamiliar weaknesses give us glimpses of mortality we would rather
avoid. The fear of death, that ultimate and universal fear, surely has a hand
(even if only implicitly) in motivating the search for ways to slow the clock.
Death is nature’s deepest and greatest barrier to total human self-mastery.
However much power and control we may come to exercise over our lives and our
environments, the time in which we may exercise that power and control is
finite, and awareness of that finitude must always make the power feel somehow
lacking. Different human societies have had very different conceptions of the
divine, but one attribute has almost universally been attached to the gods:
immortality. Our subjection to death—and our awareness of this fact—is central
to what makes us human (“mortals”) rather than divine, and it makes us fearful
and weak and constrained.
The scientific quest to slow the aging process is not
explicitly aimed at conquering death. But in taking the aging of the body as
itself a kind of disorder to be corrected, it treats man’s mortal condition as
a target for medicine, as if death were indeed rather like one of the specific
(fatal) diseases. There is no obvious end-point to the quest for ageless
bodies: after all, why should any lifespan, however long, be long enough? In
principle, the quest for any age-retardation suggests no inherent stopping
point, and therefore, in the extreme case, it is difficult to distinguish it
from a quest for endless life. It seeks to overcome the ephemeral nature of the
human body, and to replace it with permanent facility and endless youth.ii
The finitude of our power, and of our time, is part and
parcel of our being embodied living creatures. An ageless body is almost a
contradiction in terms, since all physical things necessarily decay over time,
and so experience the passing of time in a most immediate way. To escape from
time and age would be to escape from our bodily self—and the wish for this
escape, too, inheres deeply in at least some forms of the desire for
agelessness.
In these fundamental terms, the wish for ageless bodies and
its potential fulfillment by biotechnology may be the most radical of the
subjects we address in this report. It is not only an aspiration that can carry
us past its usual and reasonable bounds by means of new technical powers; and
it is more than a desire to be always what we are only sometimes. It is, at its
core, a desire to overcome the most fundamental bounds of our humanity, and to
redefine our bodily relationship with time and with the physical world.
And yet, although supremely radical, it is at the same time
a perfectly routine desire, one which absolutely every one of us has often
felt: watching helplessly as a loved one weakens and declines; contemplating
the limits of our time here on earth; or just hearing an unfamiliar “snap” in
our back as we reach up for a rebound on the basketball court or bend over to
lift up a grandchild. The possibility that biotechnology might be able to
significantly slow the process of aging invites us to consider carefully the
meaning of this routine but radical desire.
The retardation of aging is among the most complex—both
scientifically and ethically—of the potential “nontherapeutic” or “extra-therapeutic”
uses of biotechnology, involving several different scientific avenues and
raising deeply complicated questions for individuals and society. The moral
case for living longer is very strong, and the desire to live longer speaks
powerfully to each and every one of us. But the full consequences of doing so
may not be quite so obvious.
II. Basic
Terms And Concepts
Though everybody more or less knows what aging means,
offering a concrete definition is no simple task. In one sense, aging just
refers to the passage of time in relation to us or, put another way, it
describes our passage through time. The more years we have lived, the greater
our age (and with it our cumulative experience of life). In this sense, of
course, it is absurd to speak of age-retardation, for by definition, only death
could put a stop to our increasing years. But we mean more than this by “aging.”
It encompasses not only the passage of time but also (and more so) the
biological processes of senescence that accompany that passage, and especially
the progressive degeneration that affects the body and mind, beginning in
adulthood. To clarify the discussion that follows, we offer some basic
definitions for aging and related terms:
Aging: In this chapter we shall use “aging”
synonymously with “senescence,” rather than merely to describe the increase in
the number of years a person has been alive. Aging therefore denotes the
gradual and progressive loss of various functions over time, beginning in early
adulthood, leading to decreasing health, vigor, and well-being, increasing
vulnerability to disease, and increased likelihood of death.iii
Life-Extension: An increase in the
number of years that a person remains alive. It may be accomplished by a
variety of means, including reducing causes of death among the young, combating
the diseases of the aged, or the slowing down of aging. It may involve pushing
back senescence or merely allowing an individual to survive into longer and
deeper senescence.
Age-Retardation:
The slowing down of the biological processes involved in aging, resulting in
delayed decline and degeneration and perhaps also a longer life. It is one
possible route to life-extension.
Lifespan: The verified age
at death of an individual, and therefore the strictly chronological duration of
life.
Maximum Lifespan:
The longest lifespan ever recorded for a species—in humans today it is 122.5
years.
Life Expectancy:
The average number of years of life remaining for individuals at a given age,
assuming that age-specific mortality risks remain unchanged.
Life Cycle: The series of “stages”
through which one passes in the course of life—including, among others,
infancy, childhood, adolescence, adulthood, and old age; and the overall form
given to the experience of life by the relations of these “stages” and the
transitions between them.iv
The desire for ageless bodies involves the pursuit not only
of longer lives, but also of lives that remain vigorous longer. It seeks not
only to add years to life, but also to add life to years. This double purpose
is therefore likely to be better served by certain approaches to life-extension
than by others. Life-extension may take three broad approaches: (1) efforts to
allow more individuals to live to old age by combating the causes of death
among the young and middle-aged; (2) efforts to further extend the lives of
those who already live to advanced ages by reducing the incidence and severity
of diseases and impairments of the elderly (including muscle and memory loss)
or by replacing cells, tissues, and organs damaged over time; and (3) efforts
to mitigate or retard the effects of senescence more generally by affecting the
general process (or processes) of aging, potentially increasing not only the
average but also the maximum human lifespan.
The first, particularly in the form of combating infant
mortality (mostly through improvements in basic public health, sanitation, and
immunization), is largely responsible for the great increase in lifespans in
the twentieth century, from an average life expectancy at birth of about 48
years in 1900 to an average of about 78 years in 1999 in the United States (and
even higher in some other developed nations—for instance, over 80 years in
Japan). But this approach has been so successful that almost no further gains
in average lifespan can be expected from efforts to improve the health of the
young in the developed world.v
In fact, even if, starting today, no one in the United States died before the
age of 50, average life expectancy at birth would increase by only about 3.5
years (from just over 78 to 82 years). The increasing lifespans of the
twentieth century were an extraordinary achievement, but further significant
gains in life expectancy would require a much greater feat: extending the lives
of people who already make it to old age, and eventually extending the maximum
lifespan.
The second approach, extending the life of the elderly by
combating particular causes of death or reversing damage done by senescence,
has been most actively pursued over the past several decades. In some forms, it
has already contributed to the improved health of the elderly and to moderate
extensions of life. Extreme old age already is, in many respects, a gift or
product of human artifice, and modern medicine seems likely to make it more so
and to bring further modest increases in average lifespan. But in most of its
forms this approach, too, promises relatively moderate (though surely
meaningful and much-desired) life-extension, even if it succeeds far beyond the
most optimistic of present expectations.
For instance, if diabetes, all cardiovascular diseases, and
all forms of cancer were eliminated today, life expectancy at birth in the
United States would rise to about 90 years, from the present 78. This would
certainly be a significant increase, but not one so great as to bring about
many of the social and moral consequences that might be anticipated with
significant age-retardation. It would be a much smaller increase than that
achieved in the last century. Also, it would likely not have a serious impact
on the maximum lifespan, with few if any people living longer than the current
human maximum of 122 years.
The piecemeal character of this disease-by-disease approach
contributes to what might be its most important limitation. If (on hypothesis)
it would not get at the more general physical and mental deterioration that
often comes with old age,vi
and which we more generally think of as “aging,” it would allow individuals to
live longer, but often thereby expose them further and for a longer time to the
other ravages of the general process of progressive degeneration, including
loss of strength, hampered mobility, memory problems, impairments of the
senses, and declining mental functions and any other particular age-related
declines not specifically addressed by the methods employed. Extensions of life
that do not address this general degeneration consign their beneficiaries to
the fate of the mythical Tithonus or the Struldbruggs in Swift’s Gulliver’s
Travels: degeneration without end. A number of the most promising avenues
of cutting-edge aging research—including those involving stem-cell research,
tissue and organ replacement, and, potentially some day, nanotechnology—would
likely fall into this category, as do current efforts to find treatments for
cancers, heart disease, Alzheimer disease, and other ailments. Promising though
these may be, their currently foreseeable applications do not seem likely to
significantly extend the maximum human lifespan or to fundamentally alter the
shape of the human life cycle.
Since aging is itself a major risk-factor for many of these
human diseases, if aging could be slowed, the onset of these diseases might be
greatly delayed or mitigated. For this reason, among others, it is the third
approach—direct and general age-retardation, now being actively pursued on
several paths—that, if successful, would have the most significant physical,
social, and moral consequences. If successful, age-retardation could not only
extend the average lifespan or slow down generalized senescence; it could
extend the maximum lifespan, perhaps quite significantly. Should it succeed in
doing so, it may involve heretofore-unknown changes throughout the human life
cycle. Our discussion will briefly touch on two sorts of piecemeal approaches
to combating senescence (muscle enhancement and memory improvement), but will
then focus largely on the more generalized approach to the retardation of aging
as a whole.
III.
Scientific Background
A.
Targeting Specific Deficiencies of Old Age
Two piecemeal approaches to opposing or slowing two
specific debilities of old age illustrate the potential of targeted techniques
of combating the aging of the body, and display their differences from the more
holistic efforts to retard bodily aging altogether.
1. Muscle Enhancement.
A loss of strength and muscle mass is one of the most
noticeable and significant signs of bodily senescence. With aging, we become
more sedentary and use our muscles less, and the production of growth hormone
and circulating insulin-like growth factor (IGF-1, discussed in the previous
chapter) also decreases. There is thus less IGF-1 available to keep the muscles
large, and they become smaller, weaker, and less easily repaired when injured.
In addition, aged muscle cells are apparently less responsive to the action of
IGF-1 and mIGF-1 (muscle IGF-1) so that the impact of even vigorous exercise on
muscle size and strength diminishes with age.3
This age-related muscle diminution has been given a medical-sounding name:
sarcopenia.
As we age, several things change that predispose us to the
development of sarcopenia. We either reduce the output of, and/or become more
resistant to, anabolic stimuli to muscle, such as central nervous system input,
growth hormone, estrogen, testosterone, dietary protein, physical activity, and
insulin action. The loss of alpha-motor neuron input to muscle that occurs with
age4
is believed to be a critical factor5
since nerve-cell-to-muscle-cell connections are critical to maintaining muscle
mass and strength.
A loss of muscle size and strength is a significant problem
for older persons. In addition to slowing movement and hampering some
activities, sarcopenia is associated with an increased tendency to fall and
break bones, and such falls are major causes of morbidity among the elderly.
The techniques of muscle enhancement described in the previous chapter
(including the introduction of IGF-1 genes, the use of human growth hormone,
and other approaches) seem likely (and in a number of cases have been shown in
animals) to significantly reduce age-related loss of strength and of muscle
mass.
2. Memory Enhancement.
Memory loss is another particularly agonizing consequence of
senescence, disjointing the individual from his or her past, and bringing about
not only a loss of function but a loss of faith in one’s own senses of self and
the world. Researchers have been making meaningful strides toward an
understanding of memory loss—as a discrete and specific consequence of aging.
Much of this work has been a by-product of the effort to understand and to
treat Alzheimer disease, which first expresses itself in memory loss.
For example, researchers have discovered that cholinergic
cells are “among the first to die in Alzheimer patients and that cholinergic
mechanisms may be involved in memory formation.”6
This has led to therapeutic interventions with a class of drugs called
acetylcholinesterase inhibitors. These agents block the enzyme that destroys
acetylcholine (a neurotransmitter that scientists believe is crucial to forming
memories), with the result that acetylcholine, once released, remains in the
synapse for a longer period of time. These drugs have had a real but limited
effect on improving memory in some Alzheimer patients; they can slow down or
moderate the effects of the disease, but they do not reverse the progressive
destruction of the brain.
Memory loss is not confined to patients with Alzheimer
disease, or even to the elderly. And we should not simply assume that
biotechnical interventions that address or counteract the biological causes of
specific memory diseases like Alzheimer would have a similar effect on other
elderly individuals, or would improve memory in general. As Stephen Rose
explains: “The deficits in Alzheimer Disease and other conditions relate to
specific biochemical or physiological lesions, and there is no a priori reason,
irrespective of any ethical or other arguments, to suppose that, in the absence
of pathology, pharmacological enhancement of such processes will necessarily
enhance memory or cognition, which may already be ‘set’ at psychologically
optimal levels.”7
Nonetheless, some evidence suggests that at least some
portion of the discoveries made in research on Alzheimer disease could well
prove to enhance memory in general. For instance, a recent study tested the
effect of donepezil, one of the major acetylcholinesterase inhibitors, on the
performance of middle-aged pilots. Pilots conducted seven practice flights on a
flight simulator to train them to perform a complex series of instructions.
Then half of them took the drug donepezil for thirty days, while the other half
took a placebo. When the simulator test was then repeated, the pilots who had
taken the drug retained the training better than those who had taken the placebo.8
There is also a large body of research, mostly in animals, demonstrating that “opiate
receptor antagonists” may improve memory formation by stimulating the hormones
that are typically released in response to emotionally arousing experiences.9
The remarkable complexity of the human body as a whole and
the brain in particular makes it very difficult to isolate the functions of
memory from other neuro-physiological processes (perception, attention,
arousal, etc.) with which it is interconnected. Many “non-memory drugs” or
stimulants therefore have a significant effect on memory; and many “memory
drugs” have a significant effect on other bodily functions. So, for example,
amphetamines, Ritalin, and dunking one’s hand in freezing water have a “positive
effect” on the capacity to remember new information, at least over the short term.
But these drugs or experiences work on memory only indirectly, affecting not
the specific memory systems but the other systems of the body that influence
how the different memory systems function.vii
Recent research in animals has also improved our
understanding of certain molecular and genetic “switches” that control memory.
For example, in 1990, Eric Kandel discovered that blocking the molecule CREB
(c-AMP [cyclic adenosine monophosphate] Response Element Binding protein) in
sea slug nerve cells blocked new long-term memory without affecting short-term
memory.10
A few years later, Tim Tully and Jerry Yin genetically engineered fruit flies
with the CREB molecule turned “on”; the resulting flies learned basic tasks in
one try, where for normal flies it often took ten tries or more. The hypothesis
is that “CREB helps turn on the genes needed to produce new proteins that etch
permanent connections between nerve cells,” and that it is “in these links that
long-term memories are stored.”11
These exciting discoveries have already launched several new pharmaceutical
companies formed specifically to develop potential drugs based on this
research. In 1999, another group of researchers succeeded in genetically
engineering mice that learn tasks much more readily. They inserted into a mouse
embryo a gene that caused over-expression of a specific receptor in the outer
surface of certain brain cells, “long suspected to be one of the basic
mechanisms of memory formation” because it allows the “brain to make an
association between two events.”viii 12
Though exciting, all of this work is very preliminary; and
its significance for producing biotechnologies that might preserve or enhance
human memory remains to be determined. So far, there seems to be no efficacious
“silver pill” or “golden gene” for producing better memories, never mind one
without any countervailing biological costs. But the work continues, and its
potential ought not be dismissed.
Piecemeal interventions to combat sarcopenia, memory loss,
or any other specific aspect or consequence of aging and senescence may of
course have profound implications for the way human beings age. But inasmuch as
they mitigate one element of aging while further exposing the individual to
others, their overall result may not be simply attractive: Longer life with
improved muscles but with unimproved or ever-weaker memories might well be
undesirable. In any case, the contribution of these piecemeal interventions to
longer, more vigorous life is unlikely to be as profound as that of some
potential approaches to the systematic (body-wide) retardation of aging.
B.
General (Body-Wide) Age-Retardation
An even more significant potential route to nearly ageless
bodies involves the body-wide retardation of the aging process, now being
pursued by some researchers. The concept of general age-retardation presumes
the existence of a general organism-wide process of aging, as opposed to a
series of unconnected processes of degeneration that would have to be treated
separately. For aging as a whole to be slowed, there must be such a thing as “aging
as a whole.” Its existence has been debated by biologists for many years, but
over the last two decades experimental evidence has increasingly suggested that
a unified process of senescence does indeed exist. There is still no clear
empirically supported theoretical concept of just how aging works, but evidence
has shown that a number of techniques appear to affect the aging of a wide
variety, if not indeed all, of the body’s organs and systems. Sharp decreases
in caloric intake and a number of genetic interventions in animals (both of
which will be discussed in greater detail below) have been shown to have
dramatic effects not only on longevity, but on practically every measurable
expression of the rate of aging, including the rates of memory loss, muscle
loss, declining activity, immune-system response, and a broad range of bodily
processes that might not otherwise be conceived of as synchronized.
Even if the way in which these techniques of
age-retardation work is not fully understood, it seems increasingly plausible
that there just might be a single process (or a small number of processes) of
aging on which they do their work. The multiple effects suggest that most, if
not all, of the various phenomena of aging are deeply connected and, in
principle, could be jointly influenced by the right sorts of interventions. It
seems increasingly likely, therefore, that something like age-retardation is in
fact possible.
The most prominent techniques of age-retardation currently
under investigation fall into the following four general categories: caloric
restriction, genetic manipulations, prevention of oxidative damage, and methods
of treating the ailments of the aged that might affect age-retardation.
1. Caloric Restriction.
It has been known since the mid-1930s that substantial
reductions in the food intake of many animals (combined with nutritional
supplements to avoid malnutrition) can have a dramatic effect on lifespan. With
nearly seven decades of laboratory research, this is by far the most studied
and best-described avenue of age-retardation, though scientists still lack a
clear understanding of how it works. What is clear, however, from numerous
studies in both invertebrates and vertebrates (including mammals), is that a
reduction of food intake to about 60 percent of normal has a significant impact
not only on lifespan but also on the rate of decline of the animal’s
neurological activity, muscle functions, immune response, and nearly every
other measurable marker of aging. Moreover, it is now clear that the effect is
not a product of a diminished metabolism, as was long believed. Calorically
restricted animals do become physically smaller, but they process energy at the
same levels as members of their species on a normal diet. In fact, studies in
mice and rats suggest that caloric restriction appears to result in
significantly increased rates of spontaneous activity, including the ability to
run greater distances and to maintain a “youthful” level of activity at an age
well beyond that of non-restricted animals of the same species. (Importantly,
however, caloric restriction in animals also often results in sterility, or
reduced fertility.)
The degree of life-extension (and likely age-retardation)
achieved through caloric restriction is quite remarkable. In mice and rats,
researchers have regularly found lifespan extended by more than 30 percent, and
in some studies by more than 50 percent.13
Studies have also found significant extensions of life and signs of retarded
aging in a number of other mammalian species, including, recently, a 16-percent
increase in the lifespan of dogs.14
Studies of caloric restriction in monkeys, conducted since
the late 1980s at the National Institute on Aging, the University of Maryland,
and the University of Wisconsin, have shown comparable effects even on some of
our nearest evolutionary cousins.15
Calorically restricted monkeys retain youthful levels of several vital hormones
well into late adulthood, have lower blood pressure, and, over a fifteen-year
period, suffer substantially less chronic illness than members of their species
on normal diets. The effect on lifespan is as yet not known. Monkeys generally
live several decades, so it will be years before it is apparent whether
calorically restricted monkeys live significantly longer than others.
The biological basis for the dramatic anti-aging effects of
caloric restriction is not now well understood, in large part because of the
sheer number of changes wrought by a simple reduction in food intake. Hundreds
of discretely measurable physiological changes occur in mice and rats on
reduced diets, making cause and effect difficult to disentangle and the
processes from which age-retardation results difficult to identify. However,
researchers in the field believe that a number of new tools and techniques
available only in the last decade or so (including DNA microarrays, new types
of genetically engineered mice, and others) promise to facilitate a greater
understanding of this process, and they believe that, in the foreseeable future,
the mechanisms by which it operates might be understood, and techniques for
achieving the same ends without a diet of near-starvation may be developed.ix
2. Genetic Manipulations.
Some of the most startling and extraordinary discoveries in
age-retardation research have involved genetic mutations that have significant
impact on lifespan and on the rate of senescence. Over the past few decades,
researchers have identified single gene alterations that, in a number of
species, dramatically extend life. For example, in nematode worms, it appears
that changes in any one of at least 50 and potentially as many as 200 genes can
significantly extend life.x
Study of these mutations is enabling scientists to trace with some precision
the biochemical pathways responsible for changes in the aging rate; knowledge
of these pathways will then provide specific targets for possible age-retarding
interventions. In recent years, a few such pathways have been identified in
worms, fruit flies, and yeast, with the numerous mutant genes having their
effect on one or another of these pathways.xi
More remarkably, a number of life-extending genetic mutations have been
identified in mice, whose genetics and physiology are far more complex than
those of worms.
As long as life-extending single-gene mutations were known
only in worms and fruit flies, there was little reason to expect that they
might also occur in humans. But findings that similar biochemical pathways are
responsible for this phenomenon in both worms and mice suggest the potential
for a similar possibility in humans. For instance, in worms, flies, and mice,
an alteration in a receptor for an insulin-like growth factor (present also in
humans) has resulted in substantial increases in lifespan. It now seems possible
that the rate of aging may be governed by highly conserved general mechanisms
across many species, and that single-gene alterations that extend life may
ultimately be discovered in humans.
Most remarkable is the magnitude of life-extension that these
mutations confer. In worms, where the effect has been most dramatic, a
single-gene alteration has been shown to double lifespan, and an alteration in
two genes has nearly tripled it. In the most extreme cases, involving
particular single-gene mutations in male worms, researchers have observed a
six-fold increase in lifespan. There are, of course, enormous physiological
differences between humans and worms. Most notably, the cells of nematode worms
stop dividing in adulthood, a fact that of course has great significance for
aging. In mammals, most notably mice, the effects have been less pronounced,
but still quite significant. Increases in the normal two-year lifespan of
laboratory mice by 25 percent to even 50 percent have been reported, and
single-gene mutations combined with caloric restriction have been shown to
result in a nearly 75-percent increase in lifespan (or up to nearly
three-and-a-half years). That 75-percent extension is, to date, the greatest
increased lifespan achieved in mammals.16
Some single-gene mutations do, however, have serious side
effects, including, most commonly, sterility or reduced fertility—problems also
observed with other techniques of age-retardation—though, on the other hand,
some recent research suggests that, at least in some organisms, it may be
possible to decouple the age-retarding effects of certain mutations from the
observed diminution of fertility and reproductive fitness.17
Some single-gene differences have also been shown to decrease longevity in one
sex of a species (most notably in fruit flies) while increasing it in the
other. In addition, some of these mutations result in reduced body size and
increased susceptibility to cold.
The effects of induced age retardation on fertility and
reproductive fitness invite interesting speculation on the possible connection
between longevity and reproduction: prolongation of life for the individual may
be in tension with renewal of life through generation; conversely, fitness for
reproduction is correlated with the process of decline leading to death. The
possibility that hormonal events triggering puberty might also be involved in
accelerating senescence has also been discussed by researchers on aging.
A different approach to the genetics of age-retardation,
this one in humans, begins with knowledge gained from the study of progeria, a
very rare genetic condition that leads not to delayed but to precocious
senescence. One form of this progressive, fatal disorder, which afflicts
approximately one in eight million newborns, is now believed to result from a
single DNA base substitution in a gene on chromosome 1. This mutation leads to
abnormal formation of the protein lamin A (LMNA), a key component of the
membrane surrounding the nucleus of cells. Many victims of progeria carry the
defective LMNA gene; others carry a mutation in a gene encoding a protein that
repairs DNA damage. These findings will likely lead not only to genetic tests
and therapeutic approaches to the treatment of progeria but also, perhaps, to
new insights into the normal aging process itself. According to Dr. Francis
Collins, director of the National Human Genome Research Institute (NHGRI) and
the leader of the research team that found the LMNA gene defect, “Our
hypothesis is that LMNA may help us solve some of the great mysteries of aging.”
Conceivably, future therapies developed to alleviate symptoms of premature
aging in progeria patients may prove effective in delaying the aging process in
unafflicted human beings as well.18
Single-gene differences that affect lifespan have not been
studied for as long as caloric restriction. It is not yet clear, in this case,
whether what is involved is true age-retardation or a form of more general
extension of life. The evidence that does exist, however, suggests a
retardation of aging, and a slowing of the loss of function and of the
deterioration of tissues and cells.
3. Prevention of Oxidative Damage.
For many years, there has been ample (if indirect) evidence
that oxygen free radicals—oxygen molecules that have one unpaired electron, and
that are therefore chemically very active—produced as inevitable by-products of
the body’s various functions, cause gradual deterioration of many of the body’s
cells and tissues. These oxygen free radicals perform some important metabolic
functions, but they can also disrupt protein synthesis and repair (especially
in mitochondria) and can cause minor errors in DNA replication that accumulate
over time. Our body produces, or obtains through our diet, a number of antioxidants
(such as superoxide dismutase [SOD], catalase [CAT], vitamin E, vitamin C,
coenzyme Q10, and alpha-lipoic acid) that destroy many, but not all, of these
oxygen free radicals. The balance of oxygen free radicals and antioxidants
seems to be connected to the rate of degeneration of cells and tissues in the
body. In fact, antioxidants may be deeply involved in the operation of the
other successful age-retardation techniques in animals. For instance, the
balance between free-radical production and antioxidant activity may modulate
the impact of caloric restriction; and one specific antioxidant seems to play a
critical role in the operation of nearly all the single-gene life-extending
mutations in nematode worms. In addition, a recent study has shown that a
synthetic antioxidant can significantly extend the lifespan of mice, and the
life-extending effect of antioxidant activity in fruit flies has also been well
documented. Researchers are exploring the potential for employing both
naturally occurring and synthetic antioxidants in humans, to retard the
degeneration of cells, reduce and slow the accumulation of errors in DNA
replication, and thereby extend the human lifespan, perhaps significantly. The
study of free-radical activity will also likely inform our understanding of the
operation of other age-retardation techniques.
4. Methods of Treating the Ailments of the Aged That Might Affect Age-Retardation.
A number of techniques that do not themselves fall squarely
under the heading of age-retardation may nonetheless offer vital clues to the
nature of the aging process, and may have a significant role to play in the
operation of age-retardation techniques. These include:
a. Hormone treatments: It has
long been known that endocrine factors are closely tied to a number of the most
prominent elements of aging. The rates of production of certain hormones
(particularly testosterone and estrogen) decline sharply in one’s later years,
and these declines are closely related to the loss of muscle mass that accompanies
aging and to a series of other age-related declines. In the past fifteen years,
researchers have been investigating the possibility of slowing or, in certain
instances, reversing these effects of aging by the replenishment of certain
hormones to more youthful levels, with particular focus on human growth
hormone, dehydroepiandrosterone (DHEA), testosterone, estrogen, pregnenolone,
progesterone, and melatonin. One prominent study, conducted in 1990 and
repeated several times since, showed that men between the ages of 60 and 80 who
were injected with human growth hormone over a six-month period developed
increased muscle mass, a loss of fat, improved skin elasticity, and decreased
cholesterol levels.19
To this point, however, there has been no verifiable claim of changes in human
lifespan as a result of hormone replacement, and some researchers have
expressed doubts about the possibility of such changes.20
This approach in a certain sense falls between what we have called
age-retardation and what might be better understood as a treatment of the
symptoms of aging. The human growth hormone studies cited above, and most
similar efforts, do not appear to slow the general rate of degeneration and
loss of function, but they reverse some of their particular effects, on both
body and mind. Although the impact of such treatments does not appear to be
generalized throughout the body, hormone treatments may play an important role
in unlocking the secrets of the aging process, and in future age-retardation
techniques. (The same may be said of stem-cell treatments and other forms of
regenerative medicine.)
b. Telomere research:
Since the mid-1980s, researchers have known that telomeres—which form the tips
of chromosomes—can shorten over time as cells divide, and that eventually this
shortening causes cells to stop dividing and to die. Certain cells—germ cells,
cancer cells, some stem cells, hair follicles, and others—are able to escape
this process of degeneration with the help of an enzyme called telomerase,
which slows the erosion and shortening of telomeres. Several studies in the
1990s suggested that telomere length correlates with cell aging, so that
preventing the shortening of telomeres can slow the aging of cells, and, under
certain conditions, might do so without increasing the risk of uncontrolled
cell-growth and cancers.21
The links between cell aging and the general aging of organisms are, however,
still quite unclear. A number of particular conditions of the aged—including
wrinkling of the skin, age-related muscular degeneration, and
atherosclerosis—have been linked, in various degrees, to cellular aging and
degeneration. These studies suggest a use for the manipulation of telomeres in
counteracting and even preventing certain “symptoms” of aging, but at this
point no mechanistic link has been demonstrated between telomere length and the
general process of organismal senescence. One recent study, however, has found
a statistically significant link between shorter average telomere length and
increased rates of mortality (from a number of causes) in the elderly.22
The appearance of changes in telomere length in experiments with other
age-retardation techniques, including caloric restriction and single-gene
mutation, also suggests a potential connection, but for the moment the nature
of that connection remains unclear. The promise of telomere manipulation
appears greatest as a means of combating some afflictions of the aged, rather
than retarding aging as such.
These different avenues of age-retardation research are not
as clearly distinguished from one another as this classification suggests. In
almost all cases, the employment of one technique offers results that are relevant
for the understanding of the others. Caloric restriction seems to affect
antioxidant production; genetic alterations can affect telo-mere length.
Several of these methods have also been shown to work in tandem. Also, recent
developments and advances in the tools of cellular and molecular biology have
begun to fuse together these disparate fields. The techniques used for one are
often also used in the others.
None of these techniques has been demonstrated to increase
human lifespans or to slow the process of aging in humans. Such a demonstration
would be quite difficult to undertake, since the human lifespan is on average
between seven and eight decades. Experiments seeking to alter it would require
a great deal of time and more than one generation of researchers (as the
subjects outlived the researchers). Moreover, there are reasons to be cautious
about extrapolating from animal models to human beings, for we are not simply
more complicated versions of worms, flies, or mice.xii
Nevertheless, there is much to be learned from animal experiments, and from
planned observational studies of human populations, and the results of such
work, combined with the existence of analogous systems and processes in humans,
suggest that scientists may indeed in the future be able to retard the human
aging process and extend both the maximum and average human lifespan. Even if
the prospect is not imminent, it may not be too early to begin considering its
potential implications.
IV. Ethical
Issues
That this prospect will be welcomed seems almost
self-evident. Who among us would not want more healthy years added to his or
her life? No one truly relishes the thought of bodily degeneration or decline,
and of one’s final years marked, as Shakespeare put it, by “a moist eye, a dry
hand, a yellow cheek, a white beard, a decreasing leg, an increasing belly . .
. your voice broken, your wind short, your chin double, your wit single, and
every part about you blasted with antiquity.”23
We would probably all want to save ourselves, and even more so our loved ones,
from the fate we have seen some of our elders endure.
The desire to live longer is also clearly echoed in some
ethical ideals. It is surely one form of the true love of life and is driven by
a deep commitment to the activities and engagements to which our lives are
dedicated. Life’s end nearly always finds human beings in the midst of projects
still uncompleted, painfully aware that the world is full of wisdom they have
yet to gain and experiences they have yet to enjoy. Much that is good about
life is the result not of our finitude but of our longevity. Although some of
us may live best when we live each day as if it were our last, many of us
thrive because we live looking ahead to many days to come—making plans, laying
foundations, building our lives with the future in mind. More time to plan, more
healthy years in which to build and to enjoy what we have built, and in which
to contribute to the lives of others, would surely be a great blessing. Not
only individuals but society too might benefit, gaining much from the added
experience and wisdom of its older members. The case for living longer is, in
part, a moral case, and a strong one. Indeed, it may well be strong enough to
overwhelm any possible objections or worries.
But to know if it would overwhelm such worries, we must
identify those worries and examine them with care. Because the case for
longer—even greatly longer—life seems so strong, the worries may at first
escape our notice. Finding and pondering them leads us to suggest that any
major alteration of the human life cycle is likely to have serious consequences
beyond the mere extension of life, and to raise difficult ethical and practical
questions, both for individuals and especially for society.
In suggesting some of these questions (and for the sake of
discussion), we make several assumptions, both about the availability of
age-retarding technology and its likely effects. We assume, first, that
technology will be available to significantly retard the process of aging, of
both body and mind, and second, that this technology will be widely available
and widely used. If the first is correct, the second almost certainly will be.
Which consequences of age-retardation are most likely will depend upon the
particular techniques that become available and the effect they have on the
shape of a life. Different techniques might alter the aging process differently
and have different effects on the life cycle. Three general possibilities might
be considered: (1) the life cycle would be stretched out like a rubber band, so
that aging is slowed more or less equally at all stages of life, and
maturation, middle age, and decline extend over a greater period; (2) a holding
back of bodily decline, so that both the process of maturation and the process
of decline occur roughly in the way they do now, but the period between
them—that is, the healthy years of the prime of life—are greatly extended; and
(3) a change in the form of decline, so that, for instance, rather than a slow
and gradual loss of faculties, bodily degradation comes very quickly, and death
comes suddenly following long years of health and vigor. We shall seek to take
account of all of these possibilities, pointing to their potentially different
ethical implications where they arise.
In listing the three alternatives, we have taken the optimist’s
view, confining our attention to life-extending outcomes that many people might
find attractive. We have done this deliberately, for two reasons. First, only
such attractive outcomes are likely to be widely embraced. Second, we wish to
stipulate that people will get what they wish for, so that we may then examine
whether what they get is likely to turn out in fact to be what they wanted (the
Midas problem). Yet before proceeding to the ethical discussion, we should
insert some notes of caution. It is possible that age-retarding techniques,
like many medical interventions, will have uneven effects: they might work well
for some, not well for others, and cause serious side effects in yet others.
For example, for some recipients of greater longevity, the result might include
a much longer period of decline and debility. Indeed, the period of debility
could be lengthened not only absolutely (as it would be on the model of a
rubber band being stretched) but also relative to the whole lifespan, and, in
either case, virtually everyone who survives past eighty or ninety might come
to expect ten to fifteen years of severely diminished capacity. All the
scenarios for happy life-extension depend on technologies that will keep
all the body’s systems going for roughly the same duration, after which
time they will shut down more or less simultaneously. But what if it should
turn out that many people experience instead partial or uncoordinated increases
in vigor (stronger joints but weaker memory, more ardent desire but diminished
potency)? Given that age-retardation sets out to alter not just this organ or
that tissue but the entire (putative) coordinated biological clock of a most
complex organism, caution and modest expectations are proper leavens for zeal,
especially as the love of longer life needs little encouragement to embrace
false hopes of greater time on earth.
We divide our discussion of the ethical questions into two
sections, dealing with the effects on individuals and the effects on society
and its institutions. As will become evident, however, the distinction between
them is not always sharp.
A. Effects on the Individual
The question of the effect of age-retardation on our
individual lives must begin with a sense of what aging means in those lives.
First we must remember that aging is not just about old
age. It is a crucial part of the (nearly) lifelong process by which we reach
old age and the end of our lives. Accordingly, its product is not so much old
age and death as the life cycle itself: the form and contour of our life
experienced in time. Strange as it may seem, from the perspective of personal
experience aging defines youth almost as much as it does old age, because each
stage of our life is defined relative to the others and to the whole of life.
Age-retardation would therefore affect not only our later years, but all of our
years, in both immediate and mediated ways. For one thing, if administered
early in life, it might quite directly prolong our youthful years by slowing
down the processes of maturation. Some of the evidence from animal studies,
cited above, suggests that some of the methods that rely upon an alteration at
the outset—including genetic alteration or the mimetics of lifelong caloric
restriction—might retard aging in the young just as in the old. This might
imply an overall “stretching out” of the entire life cycle, as one stretches a
rubber band, extending the period we spend in infancy, childhood, adolescence,
in our prime and in decline, and profoundly altering our sense of the relation
between years lived and stages of life. Slower biological aging (particularly
in a culture of faster “social aging” like ours, in which children are
increasingly exposed to things that might not so long ago have been deemed
exclusively appropriate for adult life) may cause an increasing disjunction
between the maturity of the body and mind and the expectations and requirements
of life.
Even if the age-retarding technology produces no direct
bodily effects during youth, an increased maximum lifespan or even only greatly
diminished senescence in the old could very likely affect the attitudes of the
young along with those of the old. Indeed, age-retardation could affect the
young even more than the old, insofar as the attitudes of the young are shaped
by a sense of what is to come and what is to be expected of life. The great
changes in average life expectancy over the twentieth century may have already
influenced ways in which people perceive their own future, though it is a
difficult matter after the fact to determine exactly how and why. Yet the
changes resulting from those recent increases in average life expectancy
may not provide precedent for human expectations in an unprecedented world, in
which the maximum lifespan has increased significantly and many people
are living longer than anyone has ever lived before.xiii
How might such expectations be different? It is not easy to
say, and different people will no doubt react differently. But some general
observations are in order. The first concerns the “shape” of the life cycle as
a whole. Some proponents of age-retardation research use language that suggests
an image of life as a “time line,” uniform and homogeneous, rather than as a
forward-moving drama, composing different acts or stages—infancy, childhood,
adolescence, coming-of-age, adulthood, parenthood, ripeness, decline. This
would imply an understanding of life as composed of interchangeable and essentially
identical units of time, rather than composing a whole with a meaningful form
of its own, its meaning derived in part from the stages of the life cycle and
the fact that we live as links in the chain of generations. Viewed through the
prism of this chronological atomism, the prospect of adding more years to our
lives means simply having more time, more of the same. And since life is good,
more life is better. But life as lived and experienced does not present itself
homogeneously and in discrete uniform bits, and the “time of our lives,”
informed by experience past and bent toward the future, is not the homogeneous
and featureless “dimension” that is the time of physicists. Life as lived in
time may be more akin to a symphony, in which a certain temporal order—pacing
and procession, meter and momentum—governs the relationship between the parts
and the whole and, more important, gives a dynamic process its directed
character. Lived time is also shaped by memories of those who came before, and
of who we ourselves have been; it is informed by imagined future possibilities,
created by our hopes and plans for what we might yet become. The animated shape
of a whole life affects how we live every portion, and altering the shape of
that whole might therefore have far greater consequences than merely giving us
more time.
A second observation concerns the relation between aging
and death, and between age-retardation and our attitudes about mortality.
Moving the midnight hour of a human lifespan could alter human attitudes and
dispositions toward mortality and toward the whole of life. Life-extension does
not mean immortality, to be sure—if for no other reason than that the
attainment of immortality is scientifically implausible. But the impulse to
extend our lives in general, rather than to combat particular diseases or
ailments that shorten our lives, is a declaration of opposition to death as
such. In addressing aging as a disease to be cured, we are, in principle, and
at least tacitly, expressing a desire never to grow old and die, or, in a word,
a desire to live forever. There is no reason to suspect that life-extension
research would stop were we to achieve some mildly extended human lifespan,
say, to 140, or 160, or 180 years. Why would it? Having declared that our
present term of life is inadequate, why should we settle for another? A life
lived from the start under the influence of age-retarding techniques is a life
lived in express opposition to the constraints of mortality. Taken to its
extreme, the underlying impulse driving age-retardation research is, at least
implicitly, limitless, the equivalent of a desire for immortality.
These two observations are, of course, closely tied, since
the boundaries and shape of the life cycle give form and possible meaning to a
mortal life. Its virtue consists not so much in that it leads us to death, but
in that it reminds us, by its very nature, that we will someday die, and that
we must live in a way that takes heed of that reality. If we remained at our
prime, in full swing, for decade after decade, and perhaps even for a couple of
centuries, the character of our attitudes and our activities might well change
significantly. These changes could take at least six principal forms:
1.
Greater Freedom from Constraints of Time.
First is a potentially positive consequence. A
significantly greater lifespan would open up new possibilities and freedoms.
Quite simply, longer-lived individuals would have more time in the course of
their lives to explore new things and enjoy familiar ones, to gain more and
deeper experiences, to complete more projects, to engage in more activities, to
start a new course or a new career having gained much valuable experience in
earlier ones, to have a second or third or fourth chance at something they deem
important. If life is good, more life is in many ways better. Moreover, if the
prospect of dying is well out of sight, the fear of death might diminish as
well, alleviating many of the distortions this fear can produce in our lives.
2.
Commitment and Engagement.
On the other hand, the remoteness of the midnight hour
might influence negatively how we spend our days. For although the gift of
extra time is a boon, the perception of time ahead as less limited or as
indefinite may not be. All our activities are, in one way or another, informed
by the knowledge that our time is limited, and ultimately that we have only a
certain portion of years to use up. The more keenly we are aware of that fact,
the more likely we are to aspire to spend our lives in the ways we deem
most important and vital. The notion of spending a life suggests a finite
quantity of available devotion, and as economists are fond of telling us, the
scarcity of a commodity contributes to its value. The very experience of
spending a life, and of becoming spent in doing so—that is, the very
experience of aging—contributes to our sense of accomplishment and
commitment, and to our sense of the meaningfulness of time’s passage, and of
our passage through it. Being “used up” by our activities reinforces our sense
of fully living in the world. Our dedication to our activities, our engagement
with life’s callings, and our continuing interest in our projects all rely to
some degree upon a sense that we are giving of ourselves, in a process
destined to result in our complete expenditure. A life lived devoid of that
sense, or so thoroughly removed from it as to be in practice devoid of it,
might well be a life of lesser engagements and weakened commitments—a life
other than the one that we have come to understand as fully human. This is not
to say it will be worse—but it will very likely be quite different.
3.
Aspiration and Urgency.
Very much related to our sense of being used up in the
course of our lives is the sense of urgency given to life by the prospect of
foreseeable death. This may be what the Psalmist means in asking God to “teach
us to number our days, that we may get a heart of wisdom.” Many of our greatest
accomplishments are pushed along, if only subtly and implicitly, by the spur of
our finitude and the sense of having only a limited time. A far more distant
horizon, a sense of essentially limitless time, might leave us less inclined to
act with urgency. Why not leave for tomorrow what you might do today, if there
are endless tomorrows before you? Our sense of the size and shape of our
future—our “life expectancy”—is a major factor affecting how we act and think
in the present.
4.
Renewal and Children.
Perhaps most significant, and most intriguing, is the deep
connection between death and new birth. The link between longevity and
fertility is a nexus of profound and mysterious human significance. The link
appears again and again, in different forms and different arenas, both in
empirical scientific investigation and in any effort at moral analysis. Most of
the age-retardation techniques tested in animals to this point appear to result
in very significant decreases in fertility (though, as noted earlier, in some
cases the effects can be uncoupled). Various theories have been proffered to
explain this link, mostly having to do with a relationship between the
mechanisms that enable fertility and those that result in degeneration and
death. Some have even suggested that the changes connected to puberty may well
be linked to those that trigger decline. Fertility and aging may be
biologically linked. Moreover, they seem to be linked in terms of human
behavior and experience.
Throughout the twentieth century, increases in life
expectancy have been accompanied by decreases in the birth rate.xiv
Of course, increased longevity alone does not explain declining birth rates.
Increased income and economic opportunity as well as improved methods of
contraception surely play a role. But increased longevity and improved health
are surely elements of the broader cultural transformation that does explain
declining birth rates. Perhaps for the first time in human history, vast
numbers of young adults, blessed with an expectation of a long disease-free and
war-free future, are living childlessly through their most fertile years,
pursuing their own fulfillment now, but with the (often mistaken) expectation
that there will always be time enough later to start a family.
One important reason for the apparent experiential link
between longevity and childbearing seems readily intelligible: without some
presentiment of our mortality, there might be less desire for renewal. And so a
world of men and women who do not hear the biological clock ticking or do not
feel the approach of their own decline might have far less interest in
bearing—and, more important, caring for—children. Children are one answer to
mortality. But people in search of other more direct and immediate answers, or,
more to the point, people whose longer lease on life leaves them relatively
heedless of its finitude, might very well be far less welcoming of children,
and far less interested in making the sacrifices needed to promote human
renewal through the coming of new generations. Whether this would in fact occur
is an empirical question, and not all Council Members are convinced of this
connection between awareness of finitude and devotion to perpetuation. But we
all believe these are possibilities well worth contemplating.
Related to the subject of the effects of longevity on
procreation is the subject of the effects of longevity on marriage and the
resulting family connections. These topics are too large—and perhaps too
speculative—to explore here. Yet two questions may suffice to point to what may
be at stake. Would people in a world affected by age-retardation be more or
less inclined to swear lifelong fidelity “until death do us part,” if their
life expectancy at the time of marriage were eighty or a hundred more years,
rather than, as today, fifty? And would intergenerational family ties be
stronger or weaker if there were five or more generations alive at any one
time?
5.
Attitudes toward Death and Mortality.
How a greatly increased lifespan lived in good health would
affect attitudes toward death is another important matter. Certainly, the
removal of the numerous causes of premature death has diminished through much
of life the fear of untimely death, though its overall effects on our
views of mortality are less easy to discern. Yet it is possible that an
individual committed to the technological struggle against aging and decline
would be less prepared for and less accepting of death, and the least willing
to acknowledge its inevitability. Given that these technologies would not in
fact achieve immortality, but only lengthen life, they could in effect make
death even less bearable, and make their beneficiaries even more terrified of
it and obsessed with it. The fact that we might die at any time could sting
more if we were less attuned to the fact that we must die at some (more-or-less
known) time. In an era of age-retardation, we might in practice therefore live
under an even more powerful preoccupation with death, but one that leads us not
to commitment, engagement, urgency, and renewal, but rather to anxiety,
self-absorption, and preoccupation with any bodily mishap or every new
anti-senescence measure.
Much may depend on how people actually grow old and die in
a new world of increased longevity. Should the end come swiftly, with little
premonitory illness (the third of the possibilities discussed above), death
might always be regarded as untimely, unprepared for, shocking, and anxiety
about accidents or other health hazards might rise.xv
But what if, in the “stretched rubber band” sort of life cycle, the period of
debility became even more protracted and difficult than it now is? We have
already seen how, thanks to antibiotics, techniques of life-support, and
medicine’s general success in preventing quick deaths from infectious diseases,
heart attacks, and strokes, many more people are now spending prolonged periods
in decay, or subject to Alzheimer disease and other age-related degenerative
disorders. One of the costs we are already paying for the gift of longevity is
the placement of elderly citizens and their families in degrading and difficult
situations that simply were not possible in earlier times. Even a cure for
Alzheimer disease, welcome as it most surely would be, would very likely leave
some other chronic debilitating illness in command of those declining years.
Under such circumstances, death might come to seem a blessing. And in the
absence of fatal illnesses to end the misery, pressures for euthanasia and
assisted suicide might mount.
6. The
Meaning of the Life Cycle.
There is also more to the question of aging than the place
of death and mortality in our lives. Not just the specter of mortality, but
also the process of aging itself affects our lives in profound ways. Aging,
after all, is a process that mediates our passage through life, and that gives
shape to our sense of the passage of time and our own maturity and relations
with others. Age-retardation technologies make aging both more manipulable and
more controllable as explicitly a human project, and partially sever age from
the moorings of nature, time, and maturity. They put it in our hands, but make
it a less intelligible component of our full human life. Having many long,
productive years, with the knowledge of many more to come, would surely bring
joy to many of us. But in the end, these techniques could also leave the
individual somewhat unhinged from the life cycle. Without the guidance of our
biological life cycle, we would be hard-pressed to give form to our
experiential life cycle, and to make sense of what time, age, and change should
mean to us.
Any of the foregoing effects of course would most likely be
subtle, and it would be exceedingly difficult to hold them up against the
promise of longer and longer life and to expect any of us simply to reject the
offer. But in considering the offer, we must take into account the value
inherent in the human life cycle, in the process of aging, and in the knowledge
we have of our mortality as we experience it. We should recognize that
age-retardation may irreparably distort these and leave us living lives that,
whatever else they might become, are in fundamental ways different from—and
perhaps less serious or rich than—what we have to this point understood to be
truly human.
Powerful as some of these concerns are, however, from the
point of view of the individual considered in isolation, the advantages of
age-retardation may well be deemed to outweigh the dangers. But individuals
should not be considered in isolation, and the full potential meaning of
age-retardation cannot come into view until we take in the possible
consequences for society as a whole. When we do so, some of these individual concerns
become far more stark and apparent, and new concerns emerge as well.
B. Effects on Society
To begin to grasp the full implications of significant
age-retardation, we must imagine what our world would look like if the use of
such techniques became the norm. This is both a reasonable expectation and a
useful premise for analysis. If effective age-retardation technologies became
available and relatively painless and inexpensive,xvi
the vast majority of us would surely opt to use them, and they would quickly
become popular and widely employed. Moreover, viewing the effects of these
technologies in the aggregate both highlights the consequences they would have
for individuals by drawing them out and showing what they would mean on a large
scale, and allows us to see certain consequences that affect the society and
its institutions directly, and that are not just individual effects writ large.
Individual changes in attitude and outlook toward children or mortality would
have far more profound effects if they were widely shared throughout society.
And at the same time, some changes, like age distributions in the population,
only become apparent at all when we take in a view of entire communities or
societies all at once.
The full social effects of age-retardation probably would
not be evident until the first cohort to benefit from treatment began to cross
the barrier of the present maximum lifespan, but lesser consequences would
become evident much sooner, as more and more of the population survived to
older ages, and lived with the plausible expectation of doing so.
Consequences will likely be apparent at every level of
society, and in almost every institution. Among the more obvious may be effects
on work opportunities, new hires, promotions and retirement plans; housing
patterns; social and cultural attitudes and beliefs; the status of traditions;
the rate and acceptability of social change; the structure of family life and
relations between the generations; and political priorities and choices, and
the locus of rule and authority in government. The experiences of the past
century offer us some clues in this regard, though the effects of significant
increases in lifespan would likely be more radical than those we have seen as a
result of twentieth-century advances.
To paint a fuller picture, we consider the potential social
implications of age-retardation in three areas: generations and families;
innovation, change, and renewal; and the aging of society.
1.
Generations and Families.
Family life and the relations between the generations are,
quite obviously, built around the shape of the life cycle. A new generation
enters the world when its parents are in their prime. With time, as parents
pass the peak of their years and begin to make way and assist their children in
taking on new responsibilities and powers, the children begin to enter their
own age of maturity, slowly taking over and learning the ropes. In their own
season, the children bring yet another generation into the world, and stand
between their parents and their children, helped by the former in helping the
latter. The cycle of succession proceeds, and the world is made fresh with a
new generation, but is kept firmly rooted by the experience and hard-earned
wisdom of the old. The neediness of the very young and the very old puts
roughly one generation at a time at the helm, and charges it with caring for
those who are coming and those who are going. They are given the power to
command the institutions of society, but with it the responsibility for the
health and continuity of those institutions.
A society reshaped by age-retardation could certainly
benefit from the wisdom and experience of more generations of older people, and
from the peace, patience, and crucial encouragement that is often a wonderful
gift of those who are no longer forging their identity or caught up in economic
or social competition. But at the same time, generation after generation would
reach and remain in their prime for many decades.xvii
Sons might no longer surpass their fathers in vigor just as they prepared to
become fathers themselves. The mature generation would have no obvious reason
to make way for the next as the years passed, if its peak became a plateau. The
succession of generations could be obstructed by a glut of the able. The old
might think less of preparing their replacements, and the young could see
before them only layers of their elders blocking the path, and no great reason
to hurry in building families or careers—remaining functionally immature “young
adults” for decades, neither willing nor able to step into the shoes of their
mothers and fathers. Families and generational institutions would surely
reshape themselves to suit the new demographic form of society, but would that
new shape be good for the young, the old, the familial ties that bind them, the
society as a whole, or the cause of well-lived human lives?
2.
Innovation, Change, and Renewal.
The same glut might also affect other institutions, private
and public. From the small business to the city council, from the military to
the Fortune 500 corporation, generational succession might be disrupted, as the
rationale for retirement diminished. Again, these institutions would benefit
from greater experience at the top, but they might find it far more difficult
to adjust to change. With the slowing of the cycles of succession might also
come the slowing of the cycles of innovation and adaptation in these
institutions.
Cultural time is not chronological time. Beliefs and
attitudes tend to be formed early in life, and few of us can really change our
fundamental outlook once we have reached our intellectual maturity. Serious
innovation, and even just successful adaptation to change, is therefore often
the function of a new generation of leaders, with new ideas to try and a
different sense of the institution’s mission and environment. Waiting decades
for upper management to retire would surely stifle this renewing energy and
slow the pace of innovation—with costs for the institutions in question and
society as a whole.
A society’s openness and freshness might be diminished not
only because large layers of elders block paths to youthful advancement. They
might also be jeopardized more fundamentally by the psychological and
existential changes that the mere passing of time and “learning how things are”
bring to many, perhaps most, people. After a while, no matter how healthy we
are or how well placed we are socially, most of us cease to look upon the world
with fresh eyes. Familiarity and routine blunt awareness. Fewer things shock or
surprise. Disappointed hopes and broken dreams, accumulated mistakes and
misfortunes, and the struggle to meet the economic and emotional demands of
daily life can take their toll in diminished ambition, insensitivity, fatigue,
and cynicism—not in everyone, to be sure, but in many people growing older.xviii
As a general matter, a society’s aspiration, hope, freshness, boldness, and
openness depend for their continual renewal on the spirit of youth, of those to
whom the world itself is new and full of promise.
3. The
Aging of Society.
Even as the ravages of aging on the lives of individuals
were diminished, society as a whole would age. The average age of the
population would, of course, increase, and, as we have seen, the birthrate and
the inflow of the young would likely decrease. The consequences of these trends
are very difficult to forecast, and would depend to a great extent on the
character of the technique employed to retard aging. If the delay of senescence
made it more acute when it did come, then the costs of caring for the aged
would not be reduced but only put off, and perhaps increased. The trend we have
already seen in our society, whereby a greater share of private and public
resources goes to pay for the needs of the aged and a lesser share for the
needs of the young, would continue and grow. But society’s institutions could
likely adapt themselves to this new dynamic (though of course the fact that we
can adjust to something does not in itself settle the question of whether that
something is good or bad). More important is the change in societal attitudes,
and in the culture’s view of itself. Even if age-retardation actually decreased
the overall cost of caring for the old, which is not unimaginable, it would
still increase the age of society, affecting its views and priorities. The
nation might commit less of its intellectual energy and social resources to the
cause of initiating the young, and more to the cause of accommodating the old.
A society is greatly strengthened by the constant task of
introducing itself to new generations of members, and might perhaps be weakened
by the relative attenuation of that mission. A world that truly belonged to the
living—who expected to exercise their ownership into an ever-expanding
future—would be a very different, and perhaps a much diminished, world, focused
too narrowly on maintaining life and not sufficiently broadly on building a
good life. If individuals did not age, if their functions did not decline and
their horizons did not narrow, it might just be that societies would age far
more acutely, and would experience their own sort of senescence—a hardening of
the vital social pathways, a stiffening and loss of flexibility, a setting of
the ways and views, a corroding of the muscles and the sinews. This sort of
decline would be far less amenable to technological solutions.
A society reshaped in these and related ways would be a
very different place to live than any we have known before. It could offer exciting
new possibilities for personal fulfillment, and for the edifying accumulation
of individual and societal experience and wisdom. But it might also be less
accommodating of full human lives, less welcoming of new and uninitiated
members, and less focused on the purposes that reach beyond survival. If so,
retardation of aging—like sex selection, as discussed in an earlier
chapter—might turn out to be a Tragedy of the Commons, in which the sought-for
gains to individuals are undone or worse, owing to the social consequences of
granting them to everyone. Contemplating these concerns in advance forces us to
consider carefully the sort of world we wish to build, or to avert.
V. Conclusion
The prospect of effective and significant retardation of
aging—a goal we are all at first strongly inclined to welcome—is rife with
barely foreseeable consequences. We have tried to gesture toward some possible
effects, both positive and negative, though no one can claim to know what a
world remade by unprecedented longevity on a mass scale would really look like.
On its face, our effort to propose some possible concerns
about such a world is open to the charge that we have taken the present to be “the
best of all possible worlds.” Indeed, simply by raising any doubts, some may
accuse us—wrongly—of believing that the present is no longer the best of the
worlds we have known. Some questions we have raised about the social
implications of future increases in maximum lifespan might well have been
raised a century ago, were someone then to have proposed—no one, of course,
did—to increase the average life expectancy at birth by the amount in fact
realized since 1900 (thirty years, from 48 to 78). Empirical studies of the
consequences of that large increase are lacking, for obvious reasons, and it
would be virtually impossible to try to assess now the full social costs of
this widely welcomed change. Yet if there is merit in the suggestion that too
long a life, with its end out of sight and mind, might diminish its worth, one
might wonder whether we have already gone too far in increasing longevity. If
so, one might further suggest that we should, if we could, roll back at least
some of the increases made in the average human lifespan over the past century.
These remarks prompt some large questions: Is there an
optimal human lifespan and an ideal contour of a human life? If so, does it
resemble our historical lifespan (as framed and constrained by natural limits)?xix
Or does the optimal human lifespan lie in the future, to be achieved by some
yet-to-be-developed life-extending technology? Whatever the answers to these
intriguing and important questions, nothing in our inquiry ought to suggest that
the present average lifespan is itself ideal. We do not take the present (or
any specific time past) to be “the best of all possible worlds,” and we would
not favor rolling back the average lifespan even if it were doable. Although we
suggest some possible problems with substantially longer lifespans, we have not
expressed, and would not express, a wish for shorter lifespans than are now the
norm. To the contrary, all of us surely want more people to be able to enjoy
the increased longevity that the last century produced. Those previous efforts
that have increased average lifespans have done so by reducing the risks
and removing the causes of premature death, allowing many more people to
live out their biblical three-score (today, four-score) and ten. Yet during
that time, there has been relatively little increase in the maximum
human lifespan, and not many people are living longer than the longest-lived
people ever did. Although we may learn about the future by studying somewhat
similar changes in the past, the effects of changes of the past are not an
adequate guide for the radically new possibilities that age-retardation may
bring into being. Thus, to be committed, as we are, to trying to help everyone
make it through the natural human lifespan (surely a better world than the
present) does not require our being committed to altering or increasing that
lifespan. Conversely, to be concerned about the implications of departing from
a three-to-four-generational lifespan does not necessitate a reactionary embrace
of any putative virtues of premature death.
The past century’s advances in average lifespan, now
approaching eighty years for the majority of our fellow citizens, have come
about through largely intelligible operations within a natural world shaped by
human understanding and human powers. It is a conceptually manageable lifespan,
with individuals living not only through childhood and parenthood but long
enough to see their own grandchildren, and permitted a taste of each sort of
relationship. It is a world in which one’s direct family lineage is connected
by both genetics and personal experience, not so attenuated by time that
relatives feel unrelated. Generation and nurture, dependency and reciprocated
generosity, are in some harmony of proportion, and there is a pace of journey,
a coordinated coherence of meter and rhyme within the repeating cycles of
birth, ascendancy, and decline—a balance and beauty of love and renewal giving
answer to death that, however poignant, bespeaks the possibility of meaning and
goodness in the human experience. All this might be overthrown or forgotten in
the rush to fashion a technological project only along the gradient of our
open-ended desires and ambitions.
Contemplating the speculative prospect of altering the human
life cycle brings us to the crucial question: Is there a goodness and meaning
in life so fundamental that it is too wide to be grasped by our scientific
vision and too deep to be plumbed by the imperious exigencies of our natural
desire? If we go with the grain of our desires and pursue indefinite
prolongation and ageless bodies for ourselves, will we improve the parts and
heighten the present, but only at the cost of losing the coherence of an
ordered and integrated whole? Might we be cheating ourselves by departing from
the contour and constraint of natural life (our frailty and finitude), which
serve as a lens for a larger vision that might give all of life coherence and
sustaining significance? Conversely, in affirming the unfolding of birth and
growth, aging and death, might we not find access to something permanent,
something beyond this “drama of time,” something that at once transcends and
gives purpose to the processes of the earth, lifting us to a dignity beyond all
disorder, decay, and death? To raise these questions is not to answer them, but
simply to indicate the enormous matters that are at stake.
Without some connection between change and permanence, time
and the eternal, it is at best an open question whether life could be anything
but a process without purpose, a circumscribed project of purely private
significance. Our natural desires, focused on ourselves, would lead us either
to attempt to extend time as far as technologically possible or to dissolve it
in the involution of a ceaseless series of self-indulgent distractions. In
Aldous Huxley’s Brave New World, Bernard and Lenina are hovering in a
helicopter over the city, wondering how to best spend their evening together.
Lenina (typically jejune) suggests a game of electromagnetic golf. Bernard
demurs and replies, “No, that would be a waste of time.” Lenina answers back, “What’s
time for?” Only aging and death remind us that time is of the essence. They
invite us to notice that the evolution of life on earth has produced souls with
longings for the eternal and, if recognized, a chance to participate in matters
of enduring significance that ultimately could transcend time itself.
The broader issue has to do with the meaning of certain
elements of our human experience that medical science may now allow us to alter
and manipulate. The ability to retard aging puts into question the meaning of
aging in our lives, and the way we ought best to regard it: Is aging a disease?
Is it a condition to be treated or cured? Does that mean that all the generations
that have come before us have lived a life of suffering, either waiting for a
cure that never came or foolishly convincing themselves that their curse was
just a blessing in disguise? Is the finitude of human life, as our ancestors
experienced it and as our faiths and our philosophies have taught us to
understand it, really just a problem waiting to be solved? The anti-aging
medicine of the not-so-distant future would treat what we have usually thought
of as the whole, the healthy, human life as a condition to be healed. It
therefore presents us with a questionable notion both of full humanity and of
the proper ends of medicine.
The attempt to overcome aging puts in stark terms the
question that defines much of our larger investigation of the uses of
biotechnology that go beyond the treatment of the sick and wounded: Is the
purpose of medicine to make us perfect, or to make us whole? And, medicine’s
purpose aside, would we really be better off as individuals (happier and more
fulfilled) and as a society (more cultivated, more accomplished, more just) if
we had more perfect and more ageless bodies? The human being in his or her
natural wholeness is not a perfect being, and it is that very imperfection,
that never fully satisfactory relation with the world, that gives rise to our
deepest longings and our greatest accomplishments. It is what reminds us that
we are more than mere chemical machines or collections of parts, and yet that
we are less than flawless beings, seamlessly a part of and perfectly content in
a world fully under our control and direction. It is the source of some of what
we most appreciate about ourselves.
Some foreseeable biotechnologies, like those of effective
age-retardation, hold out the prospect of perfecting some among our imperfections,
and must lead us to ask just what sort of project this is that we have set
upon. Is the purpose of medicine and biotechnology, in principle, to let us
live endless, painless lives of perfect bliss? Or is their purpose rather to
let us live out the humanly full span of life within the edifying limits and
constraints of humanity’s grasp and power? As that grasp expands, and that
power increases, these fundamental questions of human purposes and ends become
more and more important, and finding the proper ways to think about them
becomes more vital but more difficult. The techniques themselves will not
answer these questions for us, and ignoring the questions will not make them go
away, even if we lived forever.
Footnotes
i. In doing so, we shall exploit the heuristic value of specific
prospects and approaches (that may or may not pan out) because we believe they
can most clearly teach us about the significance of any successful program for
retarding human aging.
ii. Some commentators, including a few members of this Council,
raise the legitimate question of whether an interest in retarding aging is, as
implied here, an (at least tacit) interest in immortality. One could, after
all, hope for a longer and hence more satisfying life or a less burdensome and
decrepit old age without ever consciously formulating a wish to live forever.
While the point is well taken, it does not refute the connection we have drawn
between the open pursuit of ageless bodies and the secret longing to overcome
death. Fear of death (however veiled and inchoate) and awareness of mortality
(however dim and confused) have long wielded a pervasive influence on much if
not all of human experience. And the founders of the modern scientific project
brought that fear and that awareness very much into the foreground when they
put forward the conquest of nature as mankind’s utmost aim. Moreover, some
contemporary scientists (though of course by no means all or most aging
researchers) do express their aspirations in these terms. For instance, in
marking the creation of the Society of Regenerative Medicine, William
Hazeltine, head of Human Genome Sciences, declared that “the real goal is to
keep people alive forever” (Science 290: 2249, 22 December 2000). We
shall carry this suggestion—as well as the serious doubts raised—with us as we
go forward.
iii. There is no clear consensus among scientists on a definition
or even a particular physical description of aging. In offering the above “definition”
we do not mean to imply a unitary phenomenon of aging, much less a unitary
cause. This description is compatible both with the notion that senescence is
due to some underlying process called “aging” and with the notion that “aging”
is a descriptive term for observable senescence, from whatever cause.
iv. The trend has not been simply linear, and indeed a notable
spike in total fertility rates occurred in the United States in the 1950s and
early 60s, but on the whole, rates declined significantly from just over 80
births per thousand women of childbearing age in 1900 to just over 50 births
per thousand women of childbearing age in 2000, while life expectancy increased
throughout the period. In addition, the unusual size of the so-called “baby
boom generation” in the United States has had to do not only with increased
birthrates in the 1950s and early 60s, but also with substantially diminished
infant mortality, that allowed more of those born to make it to adulthood.
v. Of course, this is very far from true in many less developed
nations, where mortality among the young is still very high, andwhere the
methods that served to improve health and increase lifespans in the United
States in the twentieth century still stand to do a great deal of good.
vi. Until one knows the cause or causes of aging, one cannot be
sure that piecemeal improvements would not significantly retard general
deterioration and thereby extend lifespan. Consider just one possible
explanation of aging that would suggest possible piecemeal interventions at
numerous sites. If alpha motor neuron input into muscles declines (for whatever
reason), this would lead to muscle weakness, which could lead to a more
sedentary lifestyle, which would decrease aerobic exercise, which may cause
generalized circulatory decline with a small but significant effect on tissue
perfusion (perhaps only during stress or cold), which could result in periodic
ischemia (inadequate oxygenation of tissues), which might result in cell damage
that causes slight but progressive degeneration to specific organs (for
example, kidneys, which influence blood pressure), which would add their own
imbalance and deficiencies to overall body coordination of function and
response with other “aging” effects (including maybe further decline in alpha
motor neurons). Because the organism is a single interrelated unit, anything
that adversely influences cell function can appear to be a “cause” of aging.
vii. The above description draws heavily on Steven Rose (Rose, S.,
“‘Smart drugs’: do they work, are they ethical, will they be legal?,” Nature
Reviews Neuroscience 3: 975-979, 2002). As Rose has said: “[M]emory
formation requires, amongst other cerebral processes: perception, attention,
arousal. All engage both peripheral (hormonal) and central mechanisms. Although
the processes involved in recall are less well studied it may be assumed that
it makes similar demands. Thus agents that affect any of these concomitant
processes may also function to enhance (or inhibit) cognitive performance.
Memory formation in simple learning tasks is affected by plasma steroid levels,
by adrenaline and even by glucose. At least one agent claimed to function as a
nootropic and once widely touted as a smart drug, piracetam, seems to act at
least in part via modulation of peripheral steroid levels. Central processes
too can affect performance by reducing anxiety, enhancing attention or
increasing the salience of the experience to be learned and remembered.
Amphetamines, methylphenidate (Ritalin), antidepressants, and anxiolytics
probably act in this way. Other agents regularly cited as potential smart
drugs, such as ACTH and vasopressin, may function similarly. Finally, there is
evidence from animal studies that endogenous cerebral neuromodulators such as
the neurosteroids (e.g., DHEA) and growth factors like BDNF will enhance
long-term memory for weakly acquired stimuli.” See original for complete list
of citations.
viii. The difficulty of simple and direct improvement in complex
neurological processes is underscored by the results of this experiment.
Together with some improvements in memory the mice experienced other
neurological changes, including hypersensitivity to inflammatory pain. See
Pinker, S., “Human Nature and Its Future,” presentation at the March 2003
meeting of the President’s Council on Bioethics, Washington, D.C. Transcript
available on the Council’s website, www.bioethics.gov.
ix. To reduce food consumption to 60 percent of normal, the
average active adult human being would have to lower his daily caloric intake
from 2,500 calories a day to 1,500. By any standard, that is a severely
restricted diet that few people would want to sustain for long periods.
Accordingly, much research is being devoted to the search for pharmaceuticals
(known as “caloric restriction mimetics”) that might mimic the benefits of
caloric restriction without actually forcing people to go hungry. See Lane, M.,
et al., “The Serious Search for an Anti-Aging Pill,” Scientific American
287(2): 36-41, 2002.
x. See Austad, S., “Adding Years to Life: Current Knowledge and
Future Prospects,” presentation at the December 2002 meeting of the President’s
Council on Bioethics. Transcript available on the Council’s website,
www.bioethics.gov.
xi. A number of recent studies suggest that there may be three
separate pathways affecting normal longevity: an insulin/IGF-1 pathway; a
pathway that, during early development, sets the rate of mitochondrial
respiration in ways that affect the rate of aging and behavior of the adult; and
a poorly defined pathway affected by caloric restriction. Of course, all these
pathways may converge at some “downstream” positions. See, for instance,
Dillin, A., et al., “Rates of behavior and aging specified by mitochondrial
function during development,” Science 298 (5602): 2398-2401, 2002; and
Murphy, C., et al., “Genes that act downstream of DAF-16 to influence the
lifespan of Caenorhabditis elegans,” Nature 424: 277-283, 2003.
xii. Fruit flies, roundworms, and mice are short-lived species
subject to hazardous environments and seasonal exigencies. It may simply make
sense biologically that their lifespan would be both constrained and flexibly
regulated to coordinate survival and reproduction within favorable
circumstances in a way quite different from the human lifespan. Also, they are
less complex and more genetically determined than human beings; indeed, they
are studied in part because their genetics are so predictable. Human beings
have evolved to be much longer-lived and more versatile, and have a different
overall biological strategy, one of open indeterminacy and consciously mediated
flexibility and freedom, complemented by creativity, communication, and
cultural continuity.
xiii. In this sense, life expectancy turns out to be a uniquely
useful measure. Life expectancy is a measurement, based on statistical tables
of mortality, of the number of additional years that people of some particular
age may expect to live at a given time. This seems better suited for insurance
purposes than for capturing a snapshot of longevity. And yet, life expectancy
may be distinctly useful to moral reflection and analysis, because it is a
measure of the number of years a person may expect to have yet ahead of him or
her at any moment. It is therefore a measure of the view ahead, of the expected
and anticipated years to come, which has much to do with our attitudes about
aging and death and about how to regard and what to do with the time we have
available. Many of the most significant consequences of age-retardation could
result from an increase in the number of years that people can expect to live,
and from the resulting changes in attitudes.
xiv. The great “baby boom” of the 1950s and 1960s in the United
States was not, as one might imagine, a result of substantially increased birth
rates. In 1900, the birth rate was just above 30 births per thousand
population; in 1950 (roughly the beginning of the period called the “baby boom”)
it was 24.1, and in 1965 (the end of that period) it was 18.4. It is not
increased rates of childbearing but rather extraordinary reductions in infant
mortality (allowing many more children to live to adulthood) that explain the
relative size of the generation born in those years. The birthrate has since
continued to decline,reaching approximately 15 births per thousand population
in 2001, bringing it closer to the death rate, and therefore bringing
population growth roughly into line with figures from the early twentieth
century.
xv. Montaigne puts it this way: “I notice that in proportion as I
sink into sickness, I naturally enter into a certain disdain for life. I find
that I have much more trouble digesting this resolution when I am in health
than when I have a fever. Inasmuch as I no longer cling so hard to the good
things of life when I begin to lose the use and pleasure of them, I come to
view death with much less frightened eyes. This makes me hope that the farther
I get from life and the nearer to death, the more easily I shall accept the
exchange. . . . If we fell into such a change [decrepitude] suddenly, I don’t
think we could endure it. But when we are led by Nature’s hand down a gentle
and virtually imperceptible slope, bit by bit, one step at a time, she rolls us
into this wretched state and makes us familiar with it; so that we find no
shock when youth dies within us, which in essence and in truth is a harder
death than the complete death of a languishing life or the death of old age;
inasmuch as the leap is not so cruel from a painful life as from a sweet and
flourishing life to a grievous and painful one.” (Montaigne, M., “That to
Philosophize Is to Learn to Die,” The Complete Essays of Michel Montaigne,
trans. Donald M. Frame, Stanford: Stanford University Press, 1965, p. 63.)
xvi. Other sorts of problems, involving aggravated social
stratification based on the gift of lengthened life, might emerge if the
lifespan-extending technologies were very expensive and available only to the
privileged few, as they well might be, at least initially. Such difficulties,
already anticipated in the current inequities in health care, could be much
exacerbated even short of technologies to retard senescence. The projected
opportunities for “regenerative medicine”—featuring stem-cell-based tissue
transplantation or more extensive organ replacement—may turn out to be very
expensive and available mainly to the wealthy.
xvii. Combined with patterns of decreasing family size in the
West, this might create a peculiar reorienting of the generational makeup of
families, with fewer children and far more and older adults, layered in
succeeding generations—the opposite of a branching family tree. A lifespan of
approximately 150 years could reasonably be expected to allow one to see his or
her great-great-great-great-grandchild. But this child would have as many as 63
other such great-great-great-great-grandparents, along with 32
great-great-great-grandparents, 16 great-great-grandparents, eight
great-grandparents, four grandparents and two parents—and, if certain
demographic trends continue, few if any siblings, uncles and aunts, or cousins.
xviii. As Aristotle noted in his remarkable portrait of the old,
the young, and those in their prime, the old often “aspire to nothing great and
exalted and crave the mere necessities and comforts of existence.” (Aristotle, Rhetoric,
Book II, Ch. 13, 1389b22, trans. L. Cooper, Englewood Cliffs, N.J.:
Prentice-Hall, 1960, p. 135.)
xix. The natural history of longevity might after all teach us
something about the value of extended life. Lifespans have increased
dramatically through evolution, and apparently to great advantage. Contemporary
species are the products of evolutionary changes that have likely included
something on the order of 1,000-fold increases of lifespan since the very
short-lived earliest living forms. If increased longevity were inherently
detrimental, we humans would not have evolved to have both great abilities and
long lifespans. This result of natural and enormously gradual evolutionary
change, however, cannot in itself be taken as a reassuring precedent for any
humanly engineered change, especially if produced rapidly without the
opportunity for evolutionary testing of the resulting changes in fitness.
_______________
Endnotes
1. Olshansky, S., et al., “No truth to the Fountain of Youth,” Scientific
American, June 2002, pp. 92-95.
2. Shakespeare, W., King Henry the Fourth, Part 2, Act II,
Scene 4, 259-260.
3. Owino, V., et al., “Age-related loss of skeletal muscle
function and the ability to express the autocrine form of insulin-like growth
factor-1 (MGF) in response to mechanical overload,” FEBS Letters, 505:
259-263, 2001.
4. Brown, W., “A method for estimating the number of motor units
in thenar muscles and the changes in motor unit count with aging,” Journal
of Neurology, Neurosurgery, and Psychiatry 35: 845-852, 1972.
5. Roubenoff, R., et al., “Sarcopenia: Current concepts,” The
Journal of Gerontology, Biological and Medical Sciences, Series A, 55A,
M716-M724, 2000.
6. Rose, S., “‘Smart drugs’: do they work, are they ethical, will
they be legal?,” Nature Reviews, Neuroscience 3: 975-979, 2002. This
discussion also draws on James McGaugh’s presentation before the President’s
Council on Bioethics, October 17, 2002 (available at www.bioethics.gov).
8. Yesavage, J., et al., “Donepezil and flight simulator
performance: effects on retention of complex skills,” Neurology 59:
123-125, 9 July 2002.
9. McGaugh, J., “Significance and Remembrance: The Role of
Neuromodulatory Systems,” Psychological Science 1: 15-25, 1990.
10. Langreth, R., “Viagra for the Brain,” Forbes, 4
February 2002.
12. Wade, N., “Of Smart Mice and an Even Smarter Man,” New York
Times, September 7, 1999. See also Tsien, J., et al., “Genetic enhancement
of learning and memory in mice,” Nature 401: 63-69, 2 September 1999.
13. A useful review of caloric restriction work in animals is
Weindruch, R., et al., The Retardation of Aging and Disease by Dietary
Restriction. Springfield, IL: Charles Thomas Publishers, 1998.
14. The study of caloric restriction in dogs, conducted by
researchers at the University of Pennsylvania, the University of Illinois,
Cornell University, and Michigan State University, is expected to be published
in an upcoming issue of the Journal of the American Veterinary Medical
Association. Preliminary results were announced by the University of
Pennsylvania in September 2002.
15. Ramsey, J., et al., “Dietary restriction and aging in rhesus
monkeys: the University of Wisconsin study,” Experimental Gerontology 35
(9-10): 1131-1149, 2000.
16. These results refer to a yet-unpublished study brought to the
Council’s attention by Steven Austad in his presentation at its December 2002
meeting. (Available on the Council’s website at www.bioethics.gov.)
17. Dillin, A., et al., “Timing requirements for insulin/IGF-1
signaling in C. elegans,” Science 298(5594): 830-834, 2002.
18. See the NIH News Release, “Researchers Identify Gene for
Premature Aging,” April 16, 2003, available on the NHGRI website at
http://genome.gov/11006962; Eriksson, M., et al., “Recurrent de novo point
mutations in lamin A cause Hutchinson-Gilford progeria syndrome,” Nature
423: 293-298, 2003; and Vastag, B., “Cause of progeria’s premature aging found:
expected to provide insight into normal aging process,” Journal of the
American Medical Association 289: 2481-2482, 2003.
19. Rudman, D., et al., “Effects of human growth hormone in men
over sixty years old,” The New England Journal of Medicine 323:1-5,
1990.
21. An overview of the subject by Council Member Elizabeth
Blackburn in the journal Nature from November 2000 sheds light on this
controversial question (Blackburn, E., “Telomere states and cell fates,” Nature
408(6808): 53-56, 2000).
22. Cawthon, R., et al., “Association between telomere length in
blood and mortality in people aged 60 years or older,” Lancet 361(9355):
393-395, 2003.
23. Shakespeare, op. cit., Act I, Scene 2, 179-183.
==============================
Chapter
5. Happy Souls
Who has not wanted to escape the clutches of oppressive and
punishing memories? Or to calm the burdensome feelings of anxiety,
disappointment, and regret? Or to achieve a psychic state of pure and undivided
pleasure and joy? The satisfaction of such desires seems inseparable from our
happiness, which we pursue by right and with passion.
According to the Declaration of Independence, the right to
pursue happiness is one of the unalienable rights that belong equally to all
human beings. Indeed, the American Founders held that governments exist mainly
to safeguard this right—along with the rights to life and liberty—against those
who would seek to deny or suppress it. Life, the foundational good, is good
also because it makes liberty possible. And liberty is good both in itself and
as the prerequisite for pursuing happiness in ways that each of us may freely
choose for ourselves.i
Our interest in happiness is not, however, merely one interest among many. It
is an overarching interest in our complete and comprehensive well-being.
For this reason, the pursuit of happy souls is not simply,
in this report, just another case study. At the same time it implicates or
points to something final and all-embracing. For it is ultimately our desire
for happiness—for the fulfillment of our aspirations and the flourishing of our
lives—that leads us to seek, among other things, better children, superior
performance, and ageless bodies (and minds). Yet the contribution of those
proximate and subordinate ends to the ultimate and supreme end of happinessii
is partial and indirect. Having better and more accomplished children or a more
vigorous and well-working body surely can contribute to our happiness, but they
are not the thing itself: there are people with splendid children and perfectly
toned bodies who are nonetheless miserable. Superior performance, though
perhaps more integral to our own flourishing, is likewise not the whole story:
everything depends on how it fits into the larger psychic, moral, and spiritual
economy of our lives—what we long for and how well we attain it, and whether we
are satisfied with ourselves in relation to our ideals, aspirations, and actual
achievements and experiences.
Such self-satisfaction and sense of fulfillment are,
needless to say, not easily attained. On the contrary, obstacles to human
happiness abound, ranging from overt illnesses of brain and psyche, through
grief and guilt, shame and sorrow, to simple frustrations of hopes and plans.
Dementia, depression, disappointment, and despair are, alas, all too common,
and many—perhaps most—people are more often bent on overcoming these and other
impediments to happiness than on seeking it in its positive fullness.iii
In these efforts at peace of mind, human beings have from time immemorial
sought help from doctors and drugs. In a famous literary instance, Shakespeare’s
Macbeth entreats his doctor to free Lady Macbeth from the haunting memory of
her own guilty acts:
|
Macbeth. |
Canst thou not minister to a mind diseas’d, |
|
|
Pluck from the memory a rooted sorrow, |
|
|
Raze out the written troubles of the brain, |
|
|
And with some sweet oblivious antidote |
|
|
Cleanse the stuff’d bosom of that perilous stuff |
|
|
Which weighs upon the heart? |
|
Doctor. |
Therein the patient |
|
|
Must minister to himself. |
Ministering to oneself, however, is easier said than done,
and many people have found themselves unequal to the task without some outside
assistance. For centuries, they have made use of external agents to drown their
sorrows or lift their spirits. Alcohol, in different measures, can accomplish
both. So, too, certain naturally occurring psychotropic agents, from the
mythical lotus flower described in Homer’s Odyssey to the very real
euphoriants derived from the opium poppy. Yet until recently, biotechnological
aids to psychic flourishing have been relatively feeble and non-specific. Drugs
for soothing bad memories have been utterly lacking. And drugs to brighten mood
or raise self-esteem have been imperfect: unsafe, inadequately effective,
transient, liable to side effects, and frequently illegal or stigmatized.
Thanks to recent breakthroughs, however, the situation is changing rapidly. The
burgeoning field of neuroscience is providing new, more specific, and safer
agents to help us combat all sorts of psychic distress. Soon, doctors may have
just the “sweet oblivious antidote” that Macbeth so desired: drugs (such as
beta-adrenergic blockers) that numb the emotional sting typically associated
with our intensely bad memories, and “mood brighteners” (such as serotonin
reuptake inhibitors) that lift and stabilize our general disposition and make
us feel good (or better) about ourselves.
To be sure, these agents—and their better versions, yet to
come—are, for now at least, being developed not as means for drug-induced
happiness but rather as agents for combating major depression or preventing
post-traumatic stress disorder (PTSD). Yet once available for those purposes,
they could also be used to ease the soul and enhance the mood of nearly anyone.
Should this occur, further research and development of drugs helpful to the
direct pursuit of happier souls—surely a profitable business venture—would very
likely take place. As a result, our pursuit of happiness and our sense of
self-satisfaction will become increasingly open to direct biotechnical
intervention. Such possibilities raise many large questions.
By directly inducing changes in our subjective experience,
the new psychotropic drugs create the possibility of severing the link between
feelings of happiness and our actions and experiences in the world. Who would
need better children, superior performance, or more youthful bodies if
medication could provide the pleasure and sense of well-being that is the goal
of so many of our aspirations? Indeed, why would one need to discipline one’s
passions, refine one’s sentiments, and cultivate one’s virtues, in short, to
organize one’s soul for action in the world, when one’s aspiration to happiness
could be satisfied by drugs in a quick, consistent, and cost-effective manner?
Yet it is far from clear that feelings of contentment
severed from action in the world or from relationships with other people could
make us truly happy. Would a happiness that did not flow from what we do and
say, usually in association with others, be more than a simulacrum of that
happiness for which our souls fit us? More generally, would the pharmacological
management of our mental lives draw us toward or estrange us from the true
happiness that we seek? It is hard to answer in the abstract. In some cases, it
might bring us nearer, by restoring our natural ability to take satisfaction in
joyous events and satisfying deeds. In other cases, it might estrange us, by
substituting the mere feelings divorced from their natural and proper ground.
The currently available drugs to alter memory and mood, and
the new drugs and their uses that may be just around the corner, invite other
large questions about the character of human life. By using drugs to satisfy
more easily the enduring aspirations to forget what torments us and approach
the world with greater peace of mind, what deeper human aspirations might we
occlude or frustrate? What qualities of character may become less necessary
and, with diminished use, atrophy or become extinct, as we increasingly depend
on drugs to cope with misfortune? How will we experience our incompleteness or
understand our mortality as our ability grows to medically dissolve all sorts
of anxiety? Will the availability of drug-induced conditions of ecstatic
pleasure estrange us from the forms of pleasure that depend upon discipline and
devotion? And, going beyond the implications for individuals, what kind of a
society are we likely to have when the powers to control memory, mood, and
mental life through drugs reach their full maturity and are widely used?
On one level, as observed above, these questions are
already with us, and have been for centuries. Alcohol, marijuana, cocaine, and
other consciousness-affecting drugs offer temporary pleasures and escapes, and
they can surely alter behavior and sense of self. But the difference (or
potential difference) with the biotechnical interventions explored in this
chapter is their capacity for more precise, long-term, and sought-after
alterations in the human psyche. While current drugs may have more-or-less
predictable effects, psyche-altering agents of the future, devised unlike those
of the past on the basis of exact knowledge of the brain, will permit more
refined and effective interventions. While current drugs used in moderation may
give those who use them the feeling states they desire, these feeling states
quickly wear off and the psyche returns to normal. And while current drugs used
in excess may have long-term effects on the trajectory of one’s life, these
effects are typically destructive—not the effects we seek. Thus, while
some of the ethical questions explored in this chapter surely apply to current
drugs—which is not, of course, a reason to dismiss them—the core issues
involved with recreational drugs and new psychotropic biotechnologies are, in
important respects, psychologically and ethically distinct.
To be sure, the answers to the important questions raised
above must in some measure be speculative, at least for now. They will depend
on many factors: the pace of biotechnological developments; the range of
physiological and psychological effects of the new drugs; debatable opinions
about the hierarchy of human aspirations or the happiness most appropriate to
the human soul; and the actual consequences, individual and social, of the
drugs used and the purposes served. In due course, the answers about
consequences can be found only by careful empirical social and psychological
research. Yet figuring out which effects social scientists should investigate
requires prior reflection and thoughtful analysis of the possible
results and their likely human significance. And, despite lack of
foreknowledge, we are obliged now to address these questions to the best of our
abilities, if we wish to act responsibly regarding the biotechnical future that
we might be, willy-nilly, in the midst of creating for ourselves and our
descendants.
This chapter explores some of the questions connected with
possibilities for directly altering our psychic state of well-being, using
technologies that affect our memories (section II) or our moods and
dispositions (section III). But before turning to these prospects, we begin
with questions about the goal itself: What is a “happy soul”? As with the goals
discussed in the previous three chapters, the goal here too is fraught with
rich ambiguity.
I. What Are “Happy
Souls”?
The nature or meaning of happiness has always been a
contested matter. Near the start of his inquiry into the supreme human good,
Aristotle remarks that everyone agrees regarding its name—”happiness” or
“flourishing”—but regarding what it is, most people do not give the same
account as the wisest.1
Some equate it with pleasure, others with honor or recognition, wealth or
power, while still others locate it in virtuous deeds, love, or understanding.
Adjudicating these competing claims is, of course, beyond the scope of this
report. But a few pertinent questions about the character of happiness may
prove useful for what is to come. Is happiness a feeling, sensation, or mood,
or is it rather an activity? Is it a state of restful contentment or of focused
and energetic striving? Some people, especially those who are troubled by the
obstacles to happiness, equate it with peace of mind or an untroubled soul.
Others demand something more: not just the absence of distress or discomfort,
but a fullness or richness or flourishing of being. What, then, is the relation
between being happy and being (merely) satisfied? Between being satisfied and
being (merely) content? Between being content and being not discontent, or
between the latter and being not dissatisfied? And in the face of all the
obstacles to human happiness, isn’t it happiness enough not to be genuinely
miserable, not to be “uneasy”? Formally speaking, one might suggest that
happiness consists in a coincidence between one’s desires and one’s power to
satisfy them. But, as the well-known rejoinder has it, desires come in all
sizes: Is it better to be a pig satisfied or Socrates dissatisfied? If the
content matters as well as the form, how is happiness materially related to the
activities of love and friendship, work and play, song and worship? Are social
ties and activities important, or is happiness a purely solitary endeavor?
Whatever answers one might give to those questions, there
are two further questions especially pertinent to the present inquiry: Is
happiness a momentary matter or is it something experienced only over time, or
even only over a complete life? And how can one tell the difference between
true and false happiness, between the real thing and the mere likeness?
The first question introduces us to perplexities about the
subject or bearer of happiness, here called, for lack of a better term, “soul”—a
term no less problematic than “happiness.” By “soul” we mean something psychological
rather than theological: indeed, “soul” is the exact English translation of the
Greek psyche, a term we sometimes use directly as its equivalent, as
well as in the compounds “psychology” (“the account or science of the soul”)
and “psychiatry” (“the doctoring of the soul”). We mean here by “soul” or “psyche”
the interacting powers of “mind and heart”—powers of reason, speech,
understanding, intuition, memory, and imagination, as well as of desire,
passion, and feeling—powers that make us human, powers that we know from the
inside that we enjoy (and that dead or inanimate bodies lack). We mean also not
just these generically human powers, but our particular and unique
constellation of them, shaped by our own experiences, aspirations, attachments,
achievements, disappointments, and feelings. We mean at once that which makes
all of us human and that which makes each of us individually who we are.
Because the happiness we seek we seek for ourselves—for our self,
not for someone else’s, and for our self or embodied soul, not for our
bodies as material stuff—our happiness is bound up with our personhood and our
identity. We would not want to attain happiness (or any other object of our
desires) if the condition for attaining it required that we become someone
else, that we lose our identity in the process.
The importance of identity for happiness implies
necessarily the importance of memory. If experiencing our happiness depends
upon experiencing a stable identity, then our happiness depends also on our
memory, on knowing who we are in relation to who we have been. A person with
Alzheimer disease, no matter how cheerful his mood, we hesitate to call happy
precisely because, in some important sense, he is no longer altogether there as
himself. His actions in the present are severed, through the loss of memory,
from the actions and experiences that made him who and what he was and is.
Indeed, much of the dread of this disease is connected with the erosion of
personal identity that the loss of memory brings with it.
But if enfeebled memory can cripple identity, selectively
altered memory can distort it. Changing the content of our memories or altering
their emotional tonalities, however desirable to alleviate guilty or painful
consciousness, could subtly reshape who we are, at least to ourselves. With
altered memories we might feel better about ourselves, but it is not clear that
the better-feeling “we” remains the same as before. Lady Macbeth, cured of her
guilty torment, would remain the murderess she was, but not the
conscience-stricken being even she could not help but be.
The second question takes us directly to mood, and to its
link with the truth of things. In the pursuit of happiness, human beings have
always worried about falling for the appearance of happiness and missing its
reality. We are all too familiar with desires that lead astray, pleasures that
cause serious harm, temporary satisfactions that leave us depleted and
diminished. Yet however routinely we may mistake a fleeting sense of happiness
for the real thing, we regard distinguishing between the two as crucial to our
happiness. And for good reason. We don’t really believe that ignorance is
bliss; we say it ruefully to bolster spirits in the face of a sudden encounter
with a painful truth. We may manage to convince ourselves that cheating is
better than losing or that love based on a lie is better than no love at all.
But seldom do those who win by cheating or who love by deceiving cease to long
for the joy and fulfillment that come from winning fair and square or being
loved for who one truly is. Many stoop to fraud to obtain happiness, but none
want their feeling of flourishing itself to be fraudulent. Yet a fraudulent
happiness is just what the pharmacological management of our mental lives
threatens to confer upon us.
Anticipating the ethical analyses that come later in this
chapter, we identify a two-fold threat of fraudulent happiness. First, an
unchecked power to erase memories, brighten moods, and alter our emotional dispositions
could imperil our capacity to form a strong and coherent personal identity. To
the extent that our inner life ceases to reflect the ups and downs of daily
existence and instead operates independently of them, we dissipate our
identity, which is formed through engagement with others and through immersion
in the mix of routine and unpredictable events that constitute our lives.
Second, by disconnecting our mood and memory from what we do and experience,
the new drugs could jeopardize the fitness and truthfulness of how we live and
what we feel, as well as our ability to confront responsibly and with dignity
the imperfections and limits of our lives and those of others. Instead of
recognizing distress, anxiety, and sorrow as appropriate reflections of the
fragility of human life and inseparable from the setbacks and heartbreaks that
accompany the pursuit of happiness and the love of fellow mortals, we are
invited to treat them as diseases to be cured, perhaps one day eradicated.
Instead of recognizing contentment, pleasure, and joy as appropriate
reflections of the richness of human life and inseparable from the fulfilling
activities and attachments that are the heart of human happiness, we are
invited to treat them as ends in themselves, perhaps one day inducible at will.iv
To be sure, our emotions can play cruel tricks on us and
fail us in myriad ways. They often wax and wane without reason, and they are
not in themselves given to maintaining proper measure. And for those afflicted
by debilitating memories of traumatic events, or who chronically suffer
depression, despair, or a sense of deep unworthiness, the new drugs are likely
to prove a great boon, by repairing crucial capacities for a normal and fitting
emotional life. Nevertheless, it behooves us to explore the potential uses and
misuses of these new drugs carefully, for drugs that erase memories or alter
our temperaments and emotional outlooks deal with that which is most us, our
hearts and minds. If we, as individuals and as a society, fail to proceed
responsibly, the pharmacological management of our mental lives could seriously
impair our ability to pursue that happiness for which our hearts long and to which
our minds guide us.
II. Memory And
Happiness
At first glance, the pursuit of happiness—a forward-looking
activity—might seem to have little to do with memory—the remembrance of things
past. Yet a closer look reveals some deep connections. Could we be happy if we
were unable to remember our own past, if we lived only day-to-day, one moment
to the next? Could we be happy if we were unable to assimilate present
experience into the remembered narrative of previous experience? Could we be
happy in the absence of happy memories? Conversely, could we be happy in the
presence of terrible memories, memories so traumatic and so life-altering that
they cast a deep shadow over all that we do, today and tomorrow? As these
questions imply, both our capacity to remember—our ability to recall and
recollect—and the content of what we remember—the banked “traces” of specific
past experiences—may well be crucial to our prospects for happiness.v
A good memory is necessary even to do the little things
that contribute to our happiness: preparing the foods we like, riding a
bicycle, finding our way home or to the home of friends. Guiding us with little
conscious effort, such memories are silently yet deeply part of who we are.
Memory is also indispensable for our ability to learn new things: the name of a
new acquaintance, the title of a new book, the contours of a new place. This
forward-looking but memory-dependent readiness to capture and incorporate the
not-yet-known and the not-yet-lived makes possible new pursuits, new
associations, and new ways of getting along in the world—in a word, new ways of
becoming happy.
Memory is important not only for retaining knowledge of
what we can do. It is important also for allowing and enabling us to “know”—virtually
without any deliberate effort on our part—who we are. Our memory, by its
own activity, preserves for us the complex web of lived experiences that
furnish our sense of self: the shared memories of living side-by-side with
loved ones; the class long ago that changed our lives; the days we spent in
sickness and celebration; our finest moments and most shameful acts. The
memories and the “self” they shape are acquired over time. At each moment, our
then-existing web of memories shapes the way we face and understand our
everyday lives. But this web of memories is, paradoxically, not permanently
fixed, unlike an image recorded on a photograph. As we give new meaning to old
happenings and try to fit them within the larger narrative of our unfolding
existence, it changes over the course of life. Our experiences at age sixteen
will have a different meaning to us when remembered at age eighteen, and a very
different meaning yet again when remembered at age fifty. As we grow older,
memories become less vivid, but perhaps their significance becomes more clear;
although they are less immediate, they are now part of the larger story of who
we are. We can consciously re-examine the meaning of remembered events and, as
a result, change how they are remembered. Yet the memories themselves
set limits on how much can be re-written, and much of the “re-construction” or “re-membering”
of our remembered lives results from undirected “editorial” work.
Astonishingly, memory itself selectively retains and deletes, reconfigures and
reintegrates, the experiences that comprise who we have been and, therefore, are.
Our identity or sense of self emerges, grows, and changes. Yet, despite all the
changes, thanks to the integrating powers of memory, our identity also,
remarkably, persists as ours.
If the capacities of remembering are crucial for preserving
the “my-ness” of any happiness that comes our way, the content of the
memories are crucial for our happiness itself. We do not wish merely to
remember having had satisfying experiences; we wish to remember them with
satisfaction. We desire not only even-keeled memories, but also memories with
feeling and with sense: we relish the memory of devoted parents, of first love,
the birth of a child; we delight in recalling beautiful sights seen, good deeds
done, worthy efforts rewarded. We especially want our memories to be not simply
a sequence of disconnected experiences, but a narrative that seems to contain
some unfolding purpose, some larger point from beginning to end, some
aspiration discovered, pursued, and at least partially fulfilled.
Memory is central to human flourishing, in other words,
precisely because we pursue happiness in time, as time-bound beings. We have a past
and a future as well as a present, and being happy through time requires that
these be connected in a meaningful way. If we are to flourish as ourselves,
we must do so without abandoning or forgetting who we are or once were. Yet
because our lives are time-bound, our happiness is always incomplete—always
not-yet and on-the-way, always here but slipping away, but also always possible
again and in the future. Our happiest experiences can be revivified. And, as we
reminisce from greater distance and with more experience, even our painful
experiences can often acquire for us a meaning not in evidence when they
occurred.
The place of memory in the pursuit of happiness also
suggests something essential about human identity, a theme raised in various
places and in different ways throughout this report: namely, our identities are
formed both by what we do and by what we undergo or suffer. We actively choose
paths and do deeds fit to be remembered. But we also live through memorable
experiences that we would never have chosen—experiences we often wish never
happened at all. To some extent, these unchosen memories constrain us; though
we may regret the shadows they cast over our pursuit of happiness, we cannot
simply escape them while remaining who we really are. And yet, through the act
of remembering—the act of discerning and giving meaning to the past as it
really was—we can shape, to some degree, the meaning of our memories, both good
and bad.
The contribution of good memories to happiness, presented
in this overly rosy account, makes clear how bad memories can undermine
happiness, indeed, can cause misery. We can lose our memory through injury or
illness; we can be plagued by terrifying, shameful, or guilty memories. Even
for the fortunate and virtuous, life is not a bowl of cherries. To live, as we
emphasized in the last chapter, is to age and decline, in memory as well as in
muscle. To aspire is to risk disappointment. To love is to risk loss, and
eventually to lose what one loves altogether in death. Bad memories, present
inevitably to all of us, can not only mar present happiness; if sufficiently
grave, they can overwhelm us and crush the prospect of seeking happiness any
time in the future. Memory is not always a friend to happiness.
For this reason, people interested in happiness are
interested, among other things, in better memories. Precisely because, in order
to be happy, we need to be able to remember, we would like to find ways to keep
our memory capacity intact, against the dangers of senility. Precisely because
we desire happier memories, we might be tempted to “edit out,” if we could,
those memories that most disturb us or even to seek a new life history
entirely.vi
For understandable reasons, we might seek to restore the innocence or peace of
mind that our actions or our sufferings have disrupted.
Until recently, the prospect of altering our remembrance of
things past—and doing so with precision, getting the better memories we desire
without compromising memory as a whole—was a mere fantasy. But in the near
future that may not be so. Much memory research over the past decades has
focused on finding the causes and then the remedies for forgetfulness, in the first
instance to forestall or treat the senile dementias, but, in the second place,
to prevent also the annoying lapses of memory in the elderly and middle-aged,
who have trouble remembering, for example, where they left the house keys.
Although the field is full of promise,vii
there is little of practical value to report at the present time. Should such
remedies for failing memories be found, their use would be welcomed by most
people as a great boon. Assuming that there were no physical or mental side
effects—a large assumption—there is little obvious reason to be concerned about
the ethical or social implications.viii
Scientists have also sought ways to alter the content
and feeling tone of specific memories, with the goal of helping people
whose lives are crushed by remembered trauma. This research has yielded some
novel pharmacological interventions, still rather limited in their effect but
perhaps a harbinger of things to come, that change the way we remember the most
emotionally affecting experiences of life, specifically by “numbing” the
discomfort connected with the memory of our most painful experiences. The
capacity to alter or numb our remembrance of things past cuts to the heart of
what it means to remember in a human way, and it is this biotechnical
possibility that we focus on here. Deciding when or whether to use such biotechnical
power will require that we think long and hard about what it means to remember
truthfully, to live in time, and to seek happiness without losing or abandoning
our identity. The rest of this discussion of “memory and happiness” is an
invitation to such reflection.
A. Good Memories and Bad
If happiness requires better memories, how would we improve
them if we could? What would be an excellent or perfect memory?
The most obvious answer is “perfect recall.” An individual
with a perfect memory, forgetting nothing, would remember every fact, face, and
encounter, every mistake he ever made, every injury suffered at the hands of
others. But even a little reflection shows that indiscriminate and total recall
is not a blessing but a curse. Those who have it suffer like the Jorge Luis
Borges character, “Funes, the Memorious,” who describes his “all-too-perfect”
memory as “a garbage disposal”; or like the famous memory patient
Shereshevskii, whose photographic memory prevented him from forming normal
human relationships.2
“Perfect memory” makes those who possess it miserable and dysfunctional.
An excellent memory might instead mean the ability to remember things as they really
are or as
they actually happen. Yet mere accuracy of recall without
guidance about what
is worth remembering would burden us with an inability to separate the
important from the trivial. Perhaps, then, an excellent memory
would recall accurately only those things that are meaningful, important, or
worth remembering. Yet the significance of past events often becomes clear to
us only after much rumination in light of later experience, and what seems
trivial at one time may appear crucial at another. Neither can an excellent
memory be one that remembers only what we want to remember: sometimes
our most valuable memories are of events that were painful when they occurred,
but that on reflection teach us vital lessons.
Speaking loosely, one might suggest that remembering well
is remembering at the right pitch: neither too much, engulfing us in trivia or imprisoning
us in the past, nor too
little, losing track of life’s defining moments or of knowledge
needed for everyday life; neither with too much emotion, allowing past misfortunes to
haunt or consume us, nor with too
little emotion, recalling what is joyful, or horrible, or
inconsequential, all with the same monotone affect.
The difficulty of describing an “excellent memory” makes
this a problematic target for those seeking to improve human memory. They will
find more likely targets in the various forms of “bad” memories, which are more
easily described.
Curiously, some apparent weaknesses of memory are in fact
integral to its sound functioning; some of memory’s “vices” are inextricably
linked to its “virtues.” “Sometimes we forget the past and at other times we
distort it; some disturbing memories haunt us for years,” writes psychologist
Daniel Schacter. But these failings of memory, he suggests, are “by-products of
otherwise desirable and adaptive features of the human mind.”ix Put
differently, to isolate and seek to “cure” each of memory’s individual failures
would risk distorting the way memory works as a whole, weaving past, present,
and future together in a meaningful way.
Yet many defects of memory are not adaptive but
destructive, diminishing life, not facilitating it. Some people just have weak
memories; owing to inborn or acquired defects, they fail to develop normal
powers of memory. There is, for the foreseeable future, little anyone can do to
help these people.
A far more common problem is memory loss. Indeed,
most people gradually lose their capacity to remember (especially recent
events) as they age, but some do so much more severely. Patients with Alzheimer
disease sense early on that memory is beginning to slip away. As the disease
progresses, they suffer loss of self-consciousness itself—of life lived, people
loved, and the world once known—and cease to live as the persons they once
were. The amnesias, caused by trauma and much rarer than dementia, produce some
similar results.x
Finally, there are terrible memories, a class of
destructive memory problems most relevant to the present inquiry concerning
happy souls. These troubles result from the lived experience of dreadful events
(for example, violent crime or war) or one’s own awful deeds (for example,
betrayal of a friend or abuse of spouse or child), amplified by the harrowing
ways those events or deeds are remembered by especially vulnerable individuals.
In certain cases, traumatic memories grossly distort and disfigure the
individual’s psyche: such people are diagnosed with PTSD. In the most severe
cases, the traumatic memories cast a shadow over one’s whole life, making the
pursuit of happiness impossible.
Whereas weak memory (and weak cognition generally) limits
one’s ability to become the person one might wish to be, and lost memory
destroys one’s ability to know who one is, these traumatic memories can make it
extremely difficult to live with oneself and with one’s life as remembered. All
these “bad memories” jeopardize happiness, and, in principle, all offer
potentially worthy targets for biotechnological efforts to improve memory. But
only the last—the use of drugs to erase or blunt the emotional content of our
memories—would give rise to the most serious ethical and social questions. We
therefore confine our attention, for the remainder of this analysis, to the
emerging pharmacological means for altering our memory of traumatic events.
B. Biotechnology and Memory Alteration
It is a commonplace observation that, while some events
fade quickly from the mind, emotionally intense experiences form memories that
are peculiarly vivid and long-lasting. Not only do we recall such events long
after they happened, but the recollection is often accompanied, in some
measure, by a recurrence of the emotions aroused during the original
experience. The usefulness—but also the danger—of this natural strengthening of
emotionally charged memories was observed already by Descartes more than 350
years ago.xi
But it is only in our time that scientists have begun to understand the
mechanisms by which emotion and memory are linked.
A body of recent research on the formation of long-term
memory has established two crucial facts about this phenomenon. First,
immediately following a new experience there occurs a period of memory
consolidation, during which some memories are encoded in the brain with
more lasting impact than others. Second, strong emotional arousal is attended
by the release of certain stress hormones (such as epinephrine, also
known as adrenaline), and the presence or absence of these hormones in the
brain during the period of memory consolidation greatly affects how strong and
durable a memory is formed.
By the early 1990s, research on animals had shown that
these stress hormones enhance the encoding of memories by activating the
amygdala, a small almond-shaped region of the brain deep inside the temporal
lobe.xii
Experiments on rats showed that the memory of an experience can be strengthened
if epinephrine (which produces high arousal) is injected into the amygdala
immediately afterwards; conversely, such memory can be weakened by injecting
into the amygdala drugs (called beta-blockers)xiii
that suppress the action of epinephrine.3
Research with human subjects broadened these results and
shed further light on the neuromodulatory processes that regulate the encoding
of memories in the brain. Studies of patients with amnesia confirmed the
crucial role of the amygdala in the consolidation of emotionally charged
memories. People who have suffered damage to the amygdala typically have no
difficulty remembering recent mundane events, but they do not exhibit the enhanced
long-term memory normally produced by emotionally arousing experiences.
Furthermore, a person with a damaged amygdala will typically recall emotional
experiences without the normal repetition of the original emotion. In
healthy subjects, fearful experiences are encoded with fearful memories, but
subjects with amygdala damage often exhibit “abnormal fear response”: they have
difficulty learning to fear (and hence avoid) dangerous situations because they
do not recall fearful events with the appropriate emotion. Evidently, the
activation of the amygdala by stress hormones during highly emotional
experiences leads to the encoding of memories that are not only more persistent
but also more apt to return with the appropriate emotional accompaniment.
The results described above may help to explain what
happens when, after living through particularly horrifying experiences, some
people experience symptoms of PTSD. When a person experiences especially
shocking or violent events (such as a plane crash or bloody combat), the
release of stress hormones may be so intense that the memory-encoding system is
over-activated. The result is a consolidation of memories both far stronger and
more persistent than normal and also more apt, upon recollection, to call forth
the intense emotional response of the original experience. In such cases, each
time the person relives the traumatic memory, a new flood of stress hormones is
released, and the experience may be so emotionally intense as to be encoded as
a new experience. With time, the memories grow more recurrent and intrusive,
and the response—fear, helplessness, horror—more incapacitating. As we shall
see, drugs that might prevent or alleviate the symptoms of PTSD are among the
chief medical benefits that scientists expect from recent research in the
neurochemistry of memory formation.
In fact, the discovery of hormonal regulation of memory
formation was quickly followed up by clinical studies on human subjects
demonstrating that memory of emotional experiences can be altered
pharmacologically. In one particularly interesting series of experiments, Larry
Cahill and his colleagues showed that injections of beta-blockers can, by
inhibiting the action of stress hormones, suppress the memory-enhancing effects
of strong emotional arousal. The researchers showed their subjects a series of
slides and told them one of two stories to explain the events depicted; one
story was mundane and emotionally neutral, the other was tragic and emotionally
gripping. Two weeks later, the participants were asked to recall the story, and
those who had heard the emotionally arousing story were found—as expected—to
recall what was depicted in the slides in far greater detail than those who had
heard the mundane version. The experiment was then repeated, except that half
the participants were given an injection of the beta-blocker propranolol and
half were injected with a saline placebo one hour before the slide show. What
they found was that, after two weeks, those who had heard the more mundane
version of the story had the same level of recollection regardless of whether
they had received the beta-blocker or the placebo. But of the subjects who had
heard the more arousing version of the story, only those receiving the placebo
showed an enhanced level of recollection. Those who heard the arousing story
after receiving the beta-blocker found it extremely sad and emotional at the
time, but two weeks later they remembered it at the same emotional level as the
group that had heard the neutral story.4
Thus, taking propranolol appears to have little or no
effect on how we remember everyday or emotionally neutral information. But when
taken at the time of highly emotional experiences, propranolol appears to
suppress the normal memory-enhancing effects of emotional arousal—while leaving
the immediate emotional response unaffected. These results suggested the
possibility of using beta-blockers to help survivors of traumatic events to
reduce their intrusive—and in some cases crippling—memories of those events. In
2002 Roger K. Pitman and his colleagues published a pilot study reporting the
use of propranolol administered to emergency room patients within six hours
after a traumatic experience (mostly car accidents) and for an additional ten
days thereafter. The patients—both those taking the drug and those taking
placebos—were tested for their psychological and physiological response to a
re-telling (with related images) of the traumatic event. One month after the
event, those taking propranolol showed measurably lower incidence of PTSD
symptoms than the control group. And three months later, while the PTSD
symptoms of both groups had returned to comparable levels, the propranolol group
showed measurably lower psycho-physiological response to “internal cues (that
is, mental imagery) that symbolized or resembled the initial traumatic event.”5
This study, while very preliminary, suggests that drugs may
become available that will enable us not only to soften certain powerful
memories but to detach them from the strong emotions evoked by the original
experience. Propranolol and other currently available beta-blockers may not be
able to do the whole job,xiv
and, until more evidence is acquired, we do well to regard them as weak
precursors of subsequent drugs that might be more powerful and effective. Yet
the prospect of such “memory numbing” drugs has already elicited considerable
public interest in and concern about their potential uses in non-clinical
settings: to prepare a soldier to kill (or kill again) on the battlefield; to
dull the sting of one’s own shameful acts; to allow a criminal to numb the
memory of his or her victims.6
Some of these scenarios are perhaps far-fetched. But although the pharmacology
of memory alteration is a science still in its infancy, the significance of
this potential new power—to separate the subjective experience of memory from
the truth of the experience that is remembered—should not be underestimated. It
surely returns us to the large ethical and anthropological questions with which
we began—about memory’s role in shaping personal identity and the character of
human life, and about the meaning of remembering things that we would rather
forget and of forgetting things that we perhaps ought to remember.
C. Memory-Blunting: Ethical Analysis
If we had the power, by promptly taking a memory-altering
drug, to dull the emotional impact of what could become very painful memories,
when might we be tempted to use it? And for what reasons should we yield to or
resist the temptation?
At first glance, such a drug would seem ideally suited for
the prevention of PTSD, the complex of debilitating symptoms that sometimes
afflict those who have experienced severe trauma. These symptoms—which include
persistent re-experiencing of the traumatic event and avoidance of every
person, place, or thing that might stimulate the horrid memory’s return7—can
so burden mental life as to make normal everyday living extremely difficult, if
not impossible.xv
For those suffering these disturbing symptoms, a drug that could separate a
painful memory from its powerful emotional component would appear very welcome
indeed.
Yet the prospect of preventing (even) PTSD with
beta-blockers or other memory-blunting agents seems to be, for several reasons,
problematic. First of all, the drugs in question appear to be effective only
when administered during or shortly after a traumatic event—and thus well
before any symptoms of PTSD would be manifested. How then could we make, and
make on the spot, the prospective judgment that a particular event is
sufficiently terrible to warrant preemptive memory-blunting? Second, how shall
we judge which participants in the event merit such treatment? After
all, not everyone who suffers through painful experiences is destined to have
pathological memory effects. Should the drugs in question be given to everyone
or only to those with an observed susceptibility to PTSD, and, if the latter,
how will we know who these are? Finally, in some cases merely witnessing a
disturbing event (for example, a murder, rape, or terrorist attack) is
sufficient to cause PTSD-like symptoms long afterwards. Should we then, as soon
as disaster strikes, consider giving memory-altering drugs to all the
witnesses, in addition to those directly involved?
These questions point to other troubling implications. Use
of memory-blunters at the time of traumatic events could interfere with the
normal psychic work and adaptive value of emotionally charged memory. A primary
function of the brain’s special way of encoding memories for emotional
experiences would seem to be to make us remember important events longer and
more vividly than trivial events. Thus, by blunting their emotional impact,
beta-blockers or their successors would concomitantly weaken our recollection
of the traumatic events we have just experienced. Yet often it is important, in
the aftermath of such events, that at least someone remembers them clearly. For
legal reasons, to say nothing of deeper social and personal ones, the wisdom of
routinely interfering with the memories of trauma survivors and witnesses is
highly questionable.
If the apparent powers of memory-blunting drugs are
confirmed, some might be inclined to prescribe them liberally to all who are
involved in a sufficiently terrible event. After all, even those not destined
to come down with full-blown PTSD are likely to suffer painful recurrent
memories of an airplane crash, an incident of terrorism, or a violent combat
operation. In the aftermath of such shocking incidents, why not give everyone
the chance to remember these events without the added burden of painful
emotions? This line of reasoning might, in fact, tempt us to give beta-blockers
liberally to soldiers on the eve of combat, to emergency workers en route to a
disaster site, or even to individuals requesting prophylaxis against the shame
or guilt they might incur from future misdeeds—in general, to anyone facing an
experience that is likely to leave lasting intrusive memories.
Yet on further reflection it seems clear that not every
intrusive memory is a suitable candidate for prospective pharmacological
blunting. As Daniel Schacter has observed, “attempts to avoid traumatic
memories often backfire”:
Intrusive memories need to be acknowledged, confronted, and
worked through, in order to set them to rest for the long term. Unwelcome
memories of trauma are symptoms of a disrupted psyche that requires attention
before it can resume healthy functioning. Beta-blockers might make it easier
for trauma survivors to face and incorporate traumatic recollections, and in
that sense could facilitate long-term adaptation. Yet it is also possible that
beta-blockers would work against the normal process of recovery: traumatic
memories would not spring to mind with the kind of psychological force that
demands attention and perhaps intervention. Prescription of beta-blockers could
bring about an effective trade-off between short-term reductions in the sting
of traumatic memories and long-term increases in persistence of related
symptoms of a trauma that has not been adequately confronted.8
The point can be generalized: in the immediate aftermath of
a painful experience, we simply cannot know either the full meaning of the
experience in question or the ultimate character and future prospects of the
individual who experiences it. We cannot know how this experience will change
this person at this time and over time. Will he be cursed forever by unbearable
memories that, in retrospect, clearly should have been blunted medically? Or
will he succeed, over time, in “redeeming” those painful memories by actively
integrating them into the narrative of his life? By “rewriting” memories
pharmacologically we might succeed in easing real suffering at the risk of
falsifying our perception of the world and undermining our true identity.
Finally, the decision whether or not to use memory-blunting
drugs must be made in the absence of clearly diagnosable disease. The drug must
be taken right after a traumatic experience has occurred, and thus before the
different ways that different individuals handle the same experience has become
clear. In some cases, these interventions will turn out to have been preventive
medicine, intervening to ward off the onset of PTSD before it arrives—though it
is worth noting that we would lack even post hoc knowledge of whether any
particular now-unaffected individual, in the absence of using the drug, would
have become symptomatic.xvi
In other cases, the interventions would not be medicine at all: altering the
memory of individuals who could have lived well, even with severely painful
memories, without pharmacologically dulling the pain. Worse, in still other
cases, the use of such drugs would inoculate individuals in advance against the
psychic pain that should accompany their commission of cruel, brutal, or
shameful deeds. But in all cases, from the defensible to the dubious, the use
of such powers changes the character of human memory, by intervening directly
in the way individuals “encode,” and thus the way they understand, the
happenings of their own lives and the realities of the world around them.
Sorting out how and why this matters, and especially what it means for our idea
of human happiness, is the focus of the more particular—albeit brief—ethical
reflections that follow.
1. Remembering Fitly and Truly.
Altering the formation of emotionally powerful memories
risks severing what we remember from how we remember it and distorting the link
between our perception of significant human events and the significance of the
events themselves. It risks, in a word, falsifying our perception and
understanding of the world. It risks making shameful acts seem less shameful,
or terrible acts less terrible, than they really are.
Imagine the experience of a person who witnesses a shocking
murder. Fearing that he will be haunted by images of this event, he immediately
takes propranolol (or its more potent successor) to render his memory of the
murder less painful and intrusive. Thanks to the drug, his memory of the murder
gets encoded as a garden-variety, emotionally neutral experience. But in
manipulating his memory in this way, he risks coming to think about the murder
as more tolerable than it really is, as an event that should not sting those
who witness it. For our opinions about the meaning of our experiences are
shaped partly by the feelings evoked when we remember them. If,
psychologically, the murder is transformed into an event our witness can recall
without pain—or without any particular emotion—perhaps its moral
significance will also fade from consciousness. If so, he would in a sense have
ceased to be a genuine witness of the murder. When asked about it, he might
say, “Yes, I was there. But it wasn’t so terrible.”
This points us to a deeper set of questions about bad
memories: Would dulling our memory of terrible things make us too comfortable
with the world, unmoved by suffering, wrongdoing, or cruelty? Does not the
experience of hard truths—of the unchosen, the inexplicable, the tragic—remind
us that we can never be fully at home in the world, especially if we are to
take seriously the reality of human evil? Further, by blunting our experience
and awareness of shameful, fearful, and hateful things, might we not also risk
deadening our response to what is admirable, inspiring, and lovable? Can we
become numb to life’s sharpest sorrows without also becoming numb to its
greatest joys?
These questions point to what might be the highest cost of
making our memory of intolerable things more tolerable: Armed with new powers
to ease the suffering of bad memories, we might come to see all psychic pain as
unnecessary and in the process come to pursue a happiness that is less than
human: an unmindful happiness, unchanged by time and events, unmoved by life’s
vicissitudes. More precisely, we might come to pursue such happiness by
willingly abandoning or compromising our own truthful identities: instead of
integrating, as best we can, the troubling events of our lives into a more
coherent whole, we might just prefer to edit them out or make them less
difficult to live with than they really are.
There seems to be little doubt that some bitter memories
are so painful and intrusive as to ruin the possibility for normal experience
of much of life and the world. In such cases the impulse to relieve a crushing
burden and restore lost innocence is fully understandable: If there are some
things that it is better never to have experienced at all—things we would avoid
if we possibly could—why not erase them from the memory of those unfortunate
enough to have suffered them? If there are some things it is better never to
have known or seen, why not use our power over memory to restore a witness’s
shattered peace of mind? There is great force in this argument, perhaps
especially in cases where children lose prematurely that innocence that is
rightfully theirs.
And yet, there may be a great cost to acting
compassionately for those who suffer bad memories, if we do so by compromising
the truthfulness of how they remember. We risk having them live falsely in
order simply to cope, to survive by whatever means possible. Among the larger
falsehoods to which such practices could lead us, few are more problematic than
the extreme beliefs regarding the possibility—and impossibility—of human
control. Erring on the one side, we might come to imagine ourselves as having
more control over our memories and identities than we really do, believing that
we can be authors and editors of our memories while still remaining truly—and
true to—ourselves. Erring on the other side, we might come to imagine that we
are impotently in the grip of the past as we look to the future, believing that
we can never learn to live with this particular memory or give it new meaning.
And so we ease today’s pain, but only by foreclosing, in a certain way, the
possibility of being the kind of person who can live well with the whole truth—both
chosen and unchosen—and the kind of person who can live well as himself.
2. The Obligation to Remember.
Having truthful memories is not simply a personal matter.
Strange to say, our own memory is not merely our own; it is part of the fabric
of the society in which we live. Consider the case of a person who has suffered
or witnessed atrocities that occasion unbearable memories: for example, those
with firsthand experience of the Holocaust. The life of that individual might
well be served by dulling such bitter memories,xvii
but such a humanitarian intervention, if widely practiced, would seem deeply
troubling: Would the community as a whole—would the human race—be served by
such a mass numbing of this terrible but indispensable memory? Do those who
suffer evil have a duty to remember and bear witness, lest we all forget the
very horrors that haunt them? (The examples of this dilemma need not be quite
so stark: the memory of being embarrassed is a source of empathy for others who
suffer embarrassment; the memory of losing a loved one is a source of empathy
for those who experience a similar loss.) Surely, we cannot and should not
force those who live through great trauma to endure its painful memory for
the benefit of the rest of us. But as a community, there are certain events
that we have an obligation to remember—an obligation that falls
disproportionately, one might even say unfairly, on those who experience such
events most directly.9
What kind of people would we be if we did not “want” to remember the Holocaust,
if we sought to make the anguish it caused simply go away? And yet, what kind
of people are we, especially those who face such horrors firsthand, that we can
endure such awful memories?
The answer, in part, is that those who suffer terrible
things cannot or should not have to endure their own bad memories alone. If, as
a people, we have an obligation to remember certain terrible events truthfully,
surely we ought to help those who suffered through those events to come to
terms with their worst memories. Of course, one might see the new biotechnical
powers, developed precisely to ease the psychic pain of bad memories, as the
mark of such solidarity: perhaps it is our new way of meeting the obligation to
aid those who remember the hardest things, those who bear witness to us and for
us. But such solidarity may, in the end, prove false: for it exempts us from
the duty to suffer-with (literally, to feel com-passion for) those who
remember; it does not demand that we preserve the truth of their memories; it
attempts instead to make the problem go away, and with it the truth of the
experience in question.
3.
Memory and Moral Responsibility.
The question of how responsible we are or should be held
for our memories, especially our memory failures, is a complicated one: Are
remembering and forgetting voluntary or involuntary acts? To what extent should
a man who forgets his child in a car, by mistake, be held “morally accountable”
for his forgetting? Is remembering “something we do” or “something that happens
to us”?
Hard as these questions are, this much seems clear: Without
memory, both our own and that of others, the notion of moral responsibility
would largely unravel. In particular, the power to numb or eliminate the
psychic sting of certain memories risks eroding the responsibility we take for
our own actions—since we would never have to face the harsh judgment of our own
conscience (Lady Macbeth) or the memory of others. The risk applies both to
self-serving uses of such a power (for example, drugs taken after a criminal
act and before the next one) and to more ambiguous “social” uses (for example,
drugs taken after killing in war and before killing again). Without truthful
memory, we could not hold others or ourselves to account for what we do and who
we are. Without truthful memory, there could be no justice or even the
possibility of justice; without memory, there could be no forgiveness or the
possibility of forgiveness—all would simply be forgotten.
The desire for powers that numb our most painful memories
is largely a personal desire: to have such drugs for myself, in the service of
my own peace of mind and happiness. Yet we cannot be blind to the potentially
coercive and immoral uses—by other individuals and by the state—of biotechnical
interventions that alter how we remember and what we forget, and that indirectly
affect our well-being. Just as drugs that dull the emotional sting of certain
memories might be desired by the victim to ease his trauma, so they might be
useful to the assailant to dull his victim’s sense of being wronged. Perhaps no
one has a greater interest in blocking the painful memory of evil than the
evildoer. We also cannot ignore the potentially coercive nature of normalizing
the use of such drugs in certain occupations: that is, by making chemically
aided desensitization part of the “job description” (augmenting or replacing
existing non-chemical means of desensitization). Nor can we forget the central
place of manipulating memory in totalitarian societies, both real and imagined,
and the way such manipulation made living truthfully—and living
happily—impossible.
4. The
Soul of Memory, The Remembering Soul.
Perhaps more than any other subject in this report, memory
is puzzling. It is both central to who we are as individuals and as a society,
yet very hard to pin down—so variable in its many meanings and many
manifestations. Jane Austen may have captured this complexity best:
If any one faculty of our nature may be called more
wonderful than the rest, I do think it is memory. There seems something more
speakingly incomprehensible in the powers, the failures, the inequalities of
memory, than in any other of our intelligences. The memory is sometimes so
retentive, so serviceable, so obedient—at others, so bewildered and so weak—and
at others again, so tyrannical, so beyond control!—We are to be sure a miracle
every way—but our powers of recollecting and of forgetting, do seem peculiarly
past finding out.10
On the one hand, when considering the meaning of human
memory, we need to face the fact that there are limits to our control over who
we are and what we become. We are not free to decide everything that happens to
us; some experiences, both great joys and terrible misfortunes, simply befall
us. These experiences become part of who we are, part of our own life as
truthfully lived. And yet, we do have some measure of freedom in how we
live with such memories—the meaning we assign them, the place we give them in
the larger narrative of our lives. But this meaning is not simply arbitrary; it
must connect the truth or significance of the events themselves, as they really
were and really are, with our own continuing pursuit of a full and happy life.
In doing so, we might often be tempted to sacrifice the accuracy of our
memories for the sake of easing our pain or expanding our control over our own
psychic lives. But doing so means, ultimately, severing ourselves from reality
and leaving our own identity behind; it risks making us false, small, or
capable of great illusions, and thus capable of great decadence or great evil,
or perhaps simply willing to accept a phony contentment. We might be tempted to
alter our memories to preserve an open future—to live the life we wanted to
live before a particular experience happened to us. But in another sense, such
interventions assume that our own future is not open—that we cannot and could
never redeem the unwanted memory over time, that we cannot and could never
integrate the remembered experience with our own truthful pursuit of happiness.
In the end, we must wonder what life would be like—and what
kind of a people we would become—with only happy memories, with everything
difficult, uncertain, and hard edited out of our lives as we remembered and
understood them. We would suffer no loss, but perhaps only because we loved
feebly and cared little for what we had. We would never shudder at life’s
injustices, but perhaps only because we had little interest in justice. We
would little relish our own achievements, since we would achieve them without
any memory of hardship along the way and with no recollection of achieving in
spite of the odds. To have only happy memories would be a blessing—and a curse.
Nothing would trouble us, but we would probably be shallow people, never falling
to the depths of despair because we have little interest in the heights of
human happiness or in the complicated lives of those around us. In the end, to
have only happy memories is not to be happy in a truly human way. It is simply
to be free of misery—an understandable desire given the many troubles of life,
but a low aspiration for those who seek a truly human happiness.
III. Mood And
Happiness
Even more than memory, mood conditions and is conditioned
by our happiness. Thoughtful reflection reveals that memory is crucial to human
happiness because it links our present identity with our past deeds and
experiences; but the connection between mood and happiness (and also
unhappiness) is self-evident to all. Indeed, the content of our happiness seems
at first glance to be largely a function of our present mood: the word “happy”
is normally taken as the opposite of “sad,” and the question, “Are you happy?”
is typically understood as an inquiry about one’s mood. Yet although many
people, if asked, might say that being happy and being in a good mood are one
and the same, the truth of the matter is not so simple. If happiness were
nothing other than “good mood,” it would seem to follow that anything that
elevates one’s mood automatically increases one’s happiness. And if that were
the case, the development of safe and effective mood-elevating drugs—not only
for the clinically depressed but also for the merely sad or discontented—would
seem to herald a future blessed by ever-greater numbers of ever-happier people.
But, as we shall see, closer examination reveals that the connection between
mood and happiness is much more subtle, and the prospects for making people
happy through pharmacology are much more ambiguous.
The first complication concerns “mood” itself: what it is,
and how to think about it. Narrowly understood, “mood” refers to a frame of
mind or state of feeling: “I am feeling blue,” “I am in a grumpy mood,” or “I
am in the mood for dancing.” These more or less transient feeling states come
and go, shifting or persisting in ways over which we have only limited control.
Although they rise and fall as we prosper or fail in the things we try to do
from day to day, our moods are also at the mercy of fortune. They may be soured
by hunger, fatigue, or illness; they may be sweetened by a call from an old
friend, a kindness shown to a stranger, or a simply beautiful day; they may
soar into ecstasy at the birth of a child, they may sink into despair at the
death of a spouse.
Yet beneath our shifting moods are more pervasive and
persistent dispositions of feeling, commonly called “temperaments.”xviii
Temperament is the general orientation of “feeling,” “mood,” and “outlook” that
we bring to all experience and on which particular experiences work to produce
the various and shifting states of emotion. It is our temperament that inclines
us toward being generally upbeat or gloomy, hopeful or fearful, extroverted or
introverted, emotionally quick and mercurial or emotionally slow and
phlegmatic. Seen through the wider lens of temperament, “mood” means more than
cheerful or sad, “good mood” or “bad.” It covers the ranges between—and
combinations among—being confident and reticent, outgoing and shy, bold and
timid, engaged and apathetic, excitable and calm, irascible and easygoing,
ambitious and lazy, proud and humble. Although rooted in some combination of
inborn natural gifts and altered by nurture and experience, temperament is also
somewhat shapable through habituation into more or less stable traits of
character: depending on how we recurrently react to fearful situations, we
become more courageous, cowardly, or rash; depending on how we recurrently
react to other people, we become more amiable, unfriendly, or obsequious.
Although temperaments are centrally matters of feeling or emotion, they are
also related to awareness and thought. They will both color and be colored by
opinions and beliefs we have about the world and about ourselves. People with
unduly high expectations are probably more easily disappointed and discouraged;
people who believe that “selfish genes” govern behavior may be less troubled by
their own moral failings; people who trust in a loving and forgiving God may be
less susceptible to despair.
As these last comments indicate, mood and temperament are
not only outward-looking and responsive to worldly happenings. They are also
much connected with our inner sense of self. Animals no doubt experience
feelings of pleasure and pain, fear and calm, frustration and satisfaction, and
something that looks from the outside like spiritedness, anger, and even pride.
But it is unlikely that they harbor humankind’s explicitly judgmental feelings
of self-love, self-esteem, self-worth, self-doubt, and self-loathing,
especially as these are tied in human beings to some explicit or tacit idea
of who one thinks one is, judged in relation to who one thinks one should be
and (especially) in relation to others. Some of us are very hard on
ourselves, filled with self-criticism and doubt about self-worth at even the
smallest falling short; others of us are very self-content or even
self-indulgent, able to brush aside even large failures with what looks like
blithe indifference. Like the other temperaments, the self-regarding
dispositions are, of course, not simply inborn and fixed; cumulative life
experience, including our history of genuine successes and failures, no doubt
contributes much. But self-demanding perfectionists are unlikely to turn into
laid-back “accommodationists,” especially from life experience alone.
Accordingly, these self-regarding feelings and dispositions—no less than our
basic temperaments and supervening moods—play a major role in whether we find
satisfaction in life, or the opposite.
A second difficulty concerns the range and “spectral”
character of moods, however narrowly or broadly defined. Human moods,
temperaments, and attitudes of self-regard vary enormously in character,
intensity, and persistence, as well as in their effects on the way each of us
lives our lives. The possible combinations of particular dispositional traits
seem virtually limitless, and they defy the capacity of ordinary language to
describe them accurately and fully, even for any one individual. One
feeling or mood blends into another, and all of them admit of degree. When we
analytically separate out any one dimension for description—say, for example,
the range from cheerful to gloomy—we notice that people distribute themselves
along a full and continuous spectrum of “normal” mood states and dispositions,
and this seems true across the board.
Yet it is clear that there are many individuals who are not
emotionally normal, whose psyches are “taken over” for long periods of time by
a dominant and debilitating mood or outlook. They live in the grip of profound
sadness, hopelessness, or despair, or of panic and terror regarding social
situations, or unrelieved guilt, shame, or feelings of abject unworthiness. Not
liking the way they feel and are, sometimes suicidal and often desperate for
help, these people bring themselves (or are brought by others) to the doctor’s
door, where, fortunately, in many cases real help is increasingly available.
Indeed, vast numbers of people suffering persisting and disabling disorders of
mood and temperament are today diagnosed and treated by psychiatrists and other
physicians for numerous affective disorders, including major depression,
bipolar disorder, social anxiety disorder, obsessive-compulsive disorder, oppositional
disorder, and the like. Scientists increasingly believe that most of these
psychic disorders are—like schizophrenia—partly the product of, or at least
correlated with, certain underlying abnormalities and (partially heritable)
disorders in the brain. Yet there are at present no specific diagnostic tests
to prove the point. For this reason, it is often hard to determine whether any
given individual suffering the symptoms that define these disorders belongs
simply to the extreme end of a spectral distribution of “normal” temperaments
or rather to a separate “class” of people with a specific brain disorder. What
is, however, easy to recognize is the enormous misery these symptoms and
conditions cause, and the further fact that such patients often respond well to
so-called “mood-altering” or “mood-brightening” drugs.
The different meanings of “mood” and the wide range of
their character, both negative and positive, give rise to a third complication
regarding the relation of mood and happiness, this one regarding human
aspiration: What mood or moods, what states of feeling, what emotional outlook
on life and self do we aspire to? As one would expect, our aspirations in this
realm are many and varied. Some of us, depressed or despairing, crave merely a cessation
of pain, our troubles lifted. Some of us, bored or listless, would like spikes
of bliss—to get “high”—and some would even want that bliss perpetually, if that
were possible. Some would prefer simply peace or contentment, never to be sad
again. Some would have their dispositions brightened and stabilized,
inhibitions eased, optimism and resilience gained or restored. Some strive for
the best experiences—falling in love, attaining some honor, performing at one’s
best—in order to enjoy the good feelings and self-esteem that accompany those
experiences, whereas others would be satisfied by the feelings alone, without
actually having to endure the work, hardship, and risk of failure. As this
variety suggests, while the desire for happiness is universal, the content of
happiness is elusive, opinions and wishes varying from person to person
depending in part on “where we start,” “who we are,” and what we desire as the
things most needful. Increasingly, however, both our culture’s preoccupation
with “how we feel about ourselves,” and especially the availability of
mood-altering drugs that can change those feelings, have encouraged us to treat
“states of mind”—mood, feeling, disposition—as goals and targets that can be
separated and pursued apart from the actions and experiences they normally
accompany.
In the remainder of this discussion, and very mindful of
all the ambiguities and uncertainties involved in doing so, we will use “mood”
in the very broadest sense, to embrace the transient and supervening states of
feeling, the basic underlying temperaments, and the emotionally charged
outlooks we have on ourselves and the world. Any of them, if negative and
severe enough, mars the chance for happiness. Any of them, if sufficiently
enduring and disabling, deserves to be classified as illness or disease. All of
them are in principle subject to pharmacological intervention, if not today,
very likely sometime soon. Given the wide variety of mood-altering agents,
present and projected, and given our ignorance of the precise effect any
particular drug will bring about in any given person, we are somewhat at a loss
about what to call these chemicals: “antidepressants” seems too narrow, “mood-altering-agents”
too non-specific, “mood-elevators” or “mood-brighteners” too specialized, “euphoriants”
inaccurate.xxix
Moreover, no single name describes a drug that, in different people, can
alleviate depression, calm panic, moderate compulsions, boost confidence, or
improve self-esteem. Somewhat arbitrarily, we will use “mood-brighteners,”
despite the inaccuracy, so as to keep before us their ability not only to lift
mood but also to improve the outlook of the person, including about himself.
A. Mood-Improvement through Drugs
Whereas drugs designed to alter memory are new,
mood-altering agents are not. Alcohol and opiates have been with us for
centuries. Doctors first used lithium for its mood-stabilizing effects in the
early twentieth century. Since the 1950s, psychiatrists have used tricyclics
and monoamine-oxidase inhibitors (or their precursors) to treat depression. The
desire to use these and other technological means to take control of our mood
abides and likely will abide so long as there are human beings who wish for
happiness and do not have it. The desire being so strong and the technologies
so familiar, we have developed a network of laws, social taboos, professional
standards, and understandings of risks, both physical and moral, through which
we more or less manage the technologies’ use—though there continue to be many
casualties along the way, and alcoholism and drug abuse remain massive social
problems. Now, as rapid advances in scientific and medical research are
producing new technologies of feeling—safer, more powerful, and more specific
than any that came before—there is reason to suspect that our laws, knowledge,
and ethical practice are lagging behind our technology. So we must ask anew
what to think of the powers over mood we are in the midst of developing. The
question, if more familiar, is also more pressing than any connected with
powers over memory, for the technologies of mood-control are not only coming
but already here.
1. Mood-Brightening Agents: An Overview.
We already have at our disposal a wide range of newer
psychotropic agents useful in altering mood, some named above. But selective
serotonin reuptake inhibitors (SSRIs), such as Prozac, Paxil, Zoloft, Celexa,
Lexapro, and Effexor, stand out.xx
SSRIs are the newest and most advanced mood-brighteners available. There is
nothing futuristic about them—a recent poll suggests one in eight adult
Americans use them today, mostly as treatment for diagnosed illness11—yet
they give some sense of what mood-brightening technologies are to come, at
least in the near future. Their effects appear to be far-reaching, touching not
only those with obvious mental illness but also those in the penumbra of
depression, those with merely melancholy or inhibited temperaments, and
possibly those who are emotionally or temperamentally balanced or normal.12
But their effects and the reason for their effects are not understood with any
precision. They are fairly safe and non-addictive, and they are legal, yet
there is no consensus in America about the limits of their appropriate use. A
public conversation has begun, but only begun.13
While we will focus much of our discussion on SSRIs—with occasional turns to
other mood-elevating drugs, such as MDMA (methylenedioxy-n-methylamphetamine,
or “Ecstasy”)—we also keep in mind the prospect of more advanced
pharmacological means for altering mood in the not-too-distant future. We are
interested not in the SSRIs as such, but in the insights we might gain from
their current uses regarding the ethical and social implications of
mood-brightening pharmacology in general, today and especially tomorrow.
As we noted at the start of this chapter, medical researchers
developed SSRIs, and doctors by and large prescribe them, not to stave off
ordinary unhappiness, but to treat major depression and other emotional
problems so disabling as to indicate the presence of mental illness. For these
conditions, the drugs are true medicines of great benefit. In efforts to help
those afflicted with the worst anxieties and depressions, those sliding into
similar afflictions, and those suffering psychic pain severe enough—diagnosable
illness or not—to make claims on a doctor’s duty to save (that is, those at
risk of suicide), SSRIs are often indispensable, and patients and doctors have
every reason to use them.14 As
far as we know, most prescription and use of SSRIs are of this therapeutic
character.
Yet some doctors are prescribing mood-brighteners for
people whose troubles are not so severe and whose neurochemistry may not be
abnormal. This should not be surprising or shocking, given that the boundaries
between mental illness and misery or between mental health and happiness are
not easily drawn. Physicians are prescribing for patients with lesser and
lesser forms of depression, psychiatrist Peter Kramer has argued, precisely
because Prozac and similar drugs can give them relief, a classic case in which
the availability of a technology of cure drives, and expands, the definition of
illness.15
But whether or not diagnostic categories are being expanded, and properly or
not, two separate human enterprises—curing mental illness and pursuing
happiness—appear to be converging, because of the development of medicines so
effective that their use overshoots the illness for which they were developed
and because they aid or seem to aid the realization of ordinary human desires
for happier souls.
Also worth noting at the outset is the astonishing variety
of individual situations for which people use these drugs and the diverse
effects they have on users’ minds and lives. No single ethical inquiry can hope
to discuss, much less resolve, the questions attending every particular case of
use. Moreover, much hard-to-design empirical research would be needed to verify
whether the troubling consequences that ethical reflection identifies as
possible are in fact coming to pass. The subject is too subtle, the emotional
lives of human beings too diverse and elusively complex. Yet many of our
ethical and social questions cannot on those grounds be set aside.
The millions of Americans now taking SSRIs are probably
only the beginning. Epidemiologists widely consider depression to be undertreated
in America: according to recent studies, between 9.5 percent and 20 percent of
Americans suffer from some form of depression.16
If all were treated with mood-brighteners, one out of every five to ten people
would use them. Moreover, the rate of diagnosed depression appears to be
climbing in the United States, as in all developed countries—probably due not
just to greater reporting, but to real increase.17
At the same time, the diagnosis of depression seems to be expanding to include
lesser and lesser forms of sadness,18
while more and more conditions besides depression (social phobia,
obsessive-compulsive disorder, and many others) are being treated with
mood-brighteners.19
Although data is hard to come by, according to some reports as many as 20
percent of students on elite college campuses now take or have taken
prescription mood-brighteners.20
As these trends dovetail with new drugs still to come, whose risk and
side-effect profiles may well be increasingly gentle, use of mood-brighteners
will almost certainly expand.
In light, then, of both present actualities and future
possibilities, we need now to deepen our understanding of mood-brighteners, and
to evaluate their human costs as well as their benefits, as we strive to reach
sensible judgments about how they should be used. At stake are not only
questions of private health and happiness, but also, as we shall see, questions
regarding the character of American society.
2. Biological and Experiential Effects of SSRIs.
Assessment begins with trying to understand the effects of
SSRIs, both on the brain and on felt human experience. In both cases, we know
only a little of what we seek to know, and still less about the connection
between the biological and experiential effects.
Neurologically, what SSRIs do is alter the brain’s handling
of serotonin. Like other neurotransmitters, serotonin is released from one
neuron to bind with and thereby activate another. The brain recycles serotonin
after each release, gathering it up again by means of a “reuptake system.”
SSRIs inhibit the serotonin reuptake system, thus increasing the concentration
of serotonin available to the receiving neurons—hence the name, “serotonin
reuptake inhibitor.” (Since SSRIs inhibit serotonin reuptake without
interfering with reuptake of other neurotransmitters, we get the full name, “selective
serotonin reuptake inhibitor.”) When given to patients diagnosed with mood
disorders, SSRIs brighten or stabilize moods in most of them, presumably as a
result of the increased availability of serotonin in certain crucial places in
the brain.
Scientists do not yet know how inhibiting the reuptake of
serotonin alters the mental state. What serotonin does, how it functions, and
even whether it is a serotonin problem that causes depression in the first
place, remain largely unknown.21
Serotonin does not alter mood directly, such that more of it produces more
pleasure or confidence and less of it the opposite; that much is clear.
Serotonin is not an opiate or a euphoriant. But just what does happen when more
or less serotonin is available—whether mood is eventually reoriented by some
plastic development in the brain, or by some other downstream effect, some
subtle influence over feeling, perceiving, and thinking, or something else
entirely—is at present a mystery.xxi
Neuroscience is a young field; many of the powers it is yielding arrive in
advance of its capacity to understand them. And even if we knew more about
brain chemistry and its functional significance, it is not clear that such
knowledge would be of a sort to help ethical inquiry. How to characterize and
assess what someone’s mood becomes when it is serotonin-enabled—whether “happy”
or “calm” or “confident” or “insensible” or something else again—is outside of
strictly biological inquiry. Brain science is and likely will remain silent on
the nature and significance, in human terms, of the experienced changes
in mood that the SSRIs produce.
One effect of SSRIs is clear: they relieve a number of
disorders of mood, particularly depression. Yet the nature of these disorders
is complicated and their causes remain largely unknown. In DSM-IVxxii
the lengthy discussion of depression (like the discussions of other psychiatric
disorders) is essentially a compendium of symptoms, with no attempt at a
coherent account of the nature or causes of the illness.22
Although studies of patients’ family histories suggest an important role for
genetic predispositions and inherited susceptibilities, no underlying
biological counterpart to major depression, let alone its specific variants,
has so far been found, no broken part identified—not even a disorder in the
serotonin system.23
There is as yet no genetic or blood test, brain scan, or electroencephalogram
for diagnosing depression. The very term “depression” seems to refer not to one
thing, but to a heterogeneous collection of conditions with different symptoms,
causes, courses of illness—and responses to SSRIs.24
This last point is especially important: how serotonin affects a person appears
to depend—though few studies address the matter directly—on what the person’s
starting point is. The mentally ill and the more-or-less-healthy-but-unhappy
experience, it seems, different effects from the drugs. Those with the type of
depression seen in bipolar disorder often make a full recovery, becoming steady
in mood and capable of fitting emotional responses to all the highs, lows, and “middles”
of life. Those with something closer to ordinary sadness or grief, or those
with a melancholy or inhibited temperament, seem to have subtler responses,
though ones they still welcome. And some individuals respond to one medication
but not another, while others have no response at all.
Our attention here is mainly on the latter group, “normal”
people who want to feel “better than normal,” or at least better than they
normally do. People who take SSRIs in the absence of definite mental illness,
and the physicians who observe them, commonly report that negative feelings
such as sadness and anger do not disappear but diminish, as does the
inclination to brood over them. Loss, disappointment, and rejection still
sting, but not as much or as long, and one can cope with them with less
disturbance of mind. Sensitivity also declines, along with obsession,
compulsion, and anxiety, while self-esteem and confidence rise. Fear, too, is
reduced, and one is more easily able to experience pleasure and accept risk.
Mental agility, energy, sleep, and appetite become more regular, typically
increasing. And mood brightens—though not to the point of perpetual bliss or
anywhere near it.25
People do indeed feel better.
Still, it is hard to know what to make of this bundle of
reported effects. Speaking abstractly, one can see a certain unity to them, a
reduction of various negative feelings, an increase in positive ones, a general
moderation prevailing where once there was excess or deadness. Also, it seems
that only the “positive/negative axis” of feeling is touched: SSRIs do not
directly affect other aspects of feeling—do not impart or remove empathy, have
no direct effect on moral conscience, neither increase nor lessen one’s ability
to appreciate beauty. Might there be some way of understanding and
characterizing these effects as a whole?
One suggestion is that SSRIs alter a person’s native
temperament or affective disposition—an individual’s tendency to respond to the
circumstances and events of life in a particular emotional fashion.
Temperaments vary, for example, in characteristic intensity of emotions and
moods, from strong (or intense) to weak (or mild). While a severely stressful
event will of course provoke a strong reaction from almost anyone, some people
react more strongly (and some more mildly) to equivalent stresses,
and—important for our purposes—their tendencies to react at such a pitch are
long-lasting.xxiii
SSRIs affect this dimension of temperament: they tend to reduce the intensity
of emotional responsiveness.26
One might say that SSRIs, at base, make people calmer.xxiv
Yet “calmness” is not the only way to understand the
effects of SSRIs on mood and psychic experience. For one thing, the calmness
explanation stumbles on the example of MDMA (Ecstasy), which also makes more
serotonin available and which induces not calm but bliss, social and sensory
openness, and feelings of intense affection.xxv
27
A second view of serotonin function is that it deals with something more basic
than emotion and mood: a nondescript measure of well-being. This idea takes off
from findings in animal research, indicating that serotonin systems are active
in brains of lower organisms, organisms that almost certainly do not experience
conscious moods or emotions.xxvi
One could easily imagine how it might be useful for any organism to have an
internal gauge of its well-being—satisfaction of its needs and desires, its
social status, and the like—that would prod it to undertake actions that foster
survival and reproduction. Perhaps serotonin is part of such a gauge, a
mechanism by which organisms set their background level of felt well-being.28
A variety of human observations support the “background
level of felt well-being” thesis. With humans, as with primates, SSRIs do not
directly introduce or block emotions and moods; one can experience a variety of
emotions and moods—including negative ones—while taking them, and presumably
while enjoying elevated levels of serotonin. Also, while SSRIs change a user’s
serotonin levels within hours, they produce no experienced psychic effect for
weeks. Something subtler than direct control of emotion and mood is taking
place, something that would create tendencies toward, and shape the intensity
of, certain emotions and moods, but not simply implant them.
In this regard, it is striking that SSRIs are effective in
relieving symptoms for so many conditions: social phobia, obsessive-compulsive
disorder, post-traumatic stress disorder, generalized anxiety disorder,
premenstrual dysphoric disorder, a variety of eating disorders and sexual
compulsions, and the whole range of conditions clustered around major
depression, possibly ranging all the way from melancholic dispositions to
ordinary sadness. The emotions and moods, not to mention the causes, symptoms,
and courses of illness of these conditions, are very different. How is it that
SSRIs address them all? This broad efficacy makes sense if SSRIs establish a
background sense of well-being, for in the presence of such a sense those many
conditions could not persist; each disorder is an instance of feeling unwell,
and so each is inconsistent with a general sense of being well. It is as if
SSRIs erect the kind of healthy dispositional foundation that those blessed
with fortunate genetics and favorable environments tend to have (without the
need for drugs), below which, apart from the most crushing circumstances, one’s
despair will not fall.
A third hypothesis suggests that SSRIs can sometimes
transform personality. Consider, for example, the story of “Sally,” a patient
of psychiatrist Peter Kramer, who describes her case in Listening to Prozac.
Shy by nature, raised by depressed and inhibited parents, sexually abused by an
uncle, Sally developed an “entrenched timidity and social discomfort,” which
led to “a sameness to her life, a terrible monotony . . . a life of intolerable
bleakness.”29
It had few pleasures, no lovers or close friends, little to look forward to or
to relish, and—though she did not think of herself as depressed until
midlife—she became then not just depressed but “openly desperate.” As she wrote
to Kramer before seeing him:
I am forty-one years old. I feel angry and hurt most of the
time. I feel like my spirit has been shattered and fragmented with each piece
having been trampled on and bruised. I am very, very anxious. I am afraid of
everything, even centipedes and roaches. I keep thinking something very, very
bad is going to happen to me, some great misfortune, or that I’ll become
handicapped and have to depend on people to take care of me. I don’t know who I
am, because that person stopped growing at the age of four, and it makes me
very sad.30
Sally’s touching story is, in outline, widely shared: a
difficult environment amplifies a troubled or troublesome predisposition and
sets in motion a great unhappiness. Prozac had a dramatic effect on her. She
felt that the drug cleared her head, made her more calm and confident. With her
new assertiveness, she negotiated a promotion at work, where she had been
locked into one job for eighteen years. The changes in her social life were
positively stunning. More easygoing, more cheerful, and—most of all—unafraid at
last, she dated several men, came to love one, and married him: “an
extraordinary achievement, a sign of victory over a crippling aspect of the
self.” Sally said the Prozac had let her true personality finally emerge, the
personality deflected by hardship and inborn fear; it let her truly live for
the first time. When her doctor expressed some concerns and suggested
suspending the use of it temporarily, Sally flatly refused.
Trying to understand the nature of Sally’s transformation,
Kramer suggests that it was social inhibition, not depression or anxiety, that
led to her unhappiness and stagnation, and concludes as follows:
The vast majority of these [naturally shy] people,
including those who are outright inhibited socially, will be “normal” in
psychological terms. Most of them will be highly functional in their careers
and private lives. No one has ever called people with inhibited personality
mentally ill. The brief conclusion to this line of reasoning is that in
patients like Sally, and in many others with less dramatic stories and perhaps
with no history of depression at all, what we are changing with medication is
the infrastructure of personality. That is, Sally is able to marry on Prozac
because she has achieved chemically the interior milieu of someone born with a
different genome and exposed to a more benign world in childhood.31
Yet SSRIs do not transform personality utterly: Prozac only
changed the easily measured, gross traits of Sally’s temperament, Kramer
explains, not the “many small and consequential features that make each person
unique . . . [their] opinions, aspirations, bêtes noires, mannerisms, and
memories.”32
Sally acquired the states of feeling not of anyone, but of Sally, had Sally
been born and raised to be well.xxvii
Many psychiatrists disagree with Kramer’s conclusion,
arguing that people like Sally are chronically depressed or otherwise
disordered, and what appears to be personality change is actually just the
liberation of their true self.33
Yet, be this as it may, we may still share Kramer’s wonder at “the capacity of
modern medication to allow a person to experience, on a stable and continuous
basis, the feelings of someone with a different temperament and history.”
Indeed, in response to his critics, Kramer presents a sharp challenge to the
view that SSRIs cannot alter personality, in the process clearly articulating
this Council’s concern regarding the “beyond therapy” uses of these drugs.
Arguing that SSRIs clearly can produce dramatic improvements in people who were
once not considered ill, he insightfully suggests that this fact presents
doctors, along with society more generally, with the choice either to expand
the notion of mental illness or to see SSRIs as medicating personality.xxviii
These three accounts of what SSRIs fundamentally do—induce
calmness, provide a background sense of well-being, change personality—probably
ought not to be looked at as mutually exclusive competitors. Inducing a
background sense of well-being could be the cause of greater calm, and greater
calm in turn the cause of a transformed personality. The three could also be
identical: the difference between a background sense of well-being and a
greater sense of calm may be, at least in part, one of description, and each of
those could be understood as personality changes. The three accounts double
back, overlap, and imply one another at many points, and we can perhaps see
them as three ways of making the same change, whose results can, in summary, be
called a “brighter mood.”
This very confusion, however—the uncertainty regarding what
SSRIs do, the unclear relationship between the various accounts—is instructive
for thinking about the future of mood-brighteners, and we have dwelt on it for
this reason. Our technological powers often arrive far ahead of our capacity to
understand them. This is only partly due to the fact that researchers often
first come across a new and effective mood-altering drug by accident, and only
later learn the mechanism of its action. It is also due to the enormous
complexity of the brain and the still greater complexity of mental life. And it
is due especially to the deep and unbridgeable divide between the language of
inner experience and the language of neurochemistry, a fact that will always
bedevil efforts to understand the humanly felt import of molecular events in
the brain. The outcome: We acquire drugs that satisfy our aspirations, yet we
know not how or why. As the example of SSRIs shows, even though we are
ignorant, even though we suspect that the unknown effects of the drugs are
subtle and deep, we make substantial use of them nonetheless. The generalizable
lesson seems clear: in the years to come, SSRIs will in all likelihood become
more effective in accomplishing what they accomplish; they will be modified to
produce fewer and gentler side effects and they will be utilized more and more.
When some discovery leads to an altogether new drug with even greater powers to
satisfy our aspirations for a happier soul, it will also be used despite much
ignorance and uncertainty. Where deep human desires are present, and where the
effects of technology are so attractive, most people will prefer benefits
despite ignorance to knowledge without benefits.
B. Ethical Analysis
From an ethical perspective that gives primacy to personal
freedom and an individual’s right to pursue happiness as he or she defines it,
the use of mood-brighteners in search of a happier soul might seem at first
glance to be largely unproblematic. If we have available to us a drug that
induces a background sense of well-being, why shouldn’t we use it when we feel
unfulfilled or steadily “blue”? What could be wrong with, or even just
disquieting about, wanting to feel better about ourselves and our lives, and
availing ourselves of the necessary assistance in doing so? If we may embrace
psychotherapy for the same purpose, why should we not embrace mood-brighteners,
especially if they are not only safe but also cheaper and more effective than “talk
therapy”? Only a person utterly at peace with the world and content with
himself would be beyond temptation at the prospect of having his troubles effortlessly
eased. And even were we to resist the temptation for ourselves, we might seek
it for our unhappy children, whose sorrows are for most of us much more painful
than our own.
Yet further reflection gives rise to questions—about both
ends and means—that ought, at the very least, to give pause to anyone tempted
by the pharmacological road to happiness. For we care that our children—and
that we ourselves—have not only the sense or feeling of well-being, but
well-being itself. We desire not simply to be satisfied with ourselves and the
world, but to have this satisfaction as a result of deeds and loves and lives
worthy of such self-satisfaction. We do not want to kill our aspiration for a
better life by drowning in a self-absorbed contentment those experiences of
lack and self-discontent that serve as aspiration’s source, or those
engagements with the world and other people that serve as aspiration’s vehicle.xxxixHere,
then, lie several potential grounds of our unease about—not rejection
of—mood-elevating drugs: the prospect of mistaking some lesser substitute for
real happiness; the danger of seeking happiness at the cost of confounding our
own identity or losing our longings for the real thing; and the price to be
paid—in personal aspiration, interpersonal relations, and communal
character—should a large fraction of our society (successfully) pursue happier
souls by this inward-turning means.
1. Living Truly.
Most people seek some form of the well-being that Sally
came to experience, in her case only with the help of medication: We seek to be
confident in everyday life, to form lasting and meaningful relationships with
others, to pursue worthy goals and take pleasure in their achievement. But what
is the significance in relying on mood-brightening drugs to achieve such
happiness? To what extent is the happiness of the happy person attributable to
the drug and to what extent is it “her own”? To what extent are drug-induced
psychic states connected with or disconnected from life as really lived?
Surely, for Sally and others who benefit greatly from mood-brightening drugs,
the drugs are not the direct cause of their happiness. Sally’s happiness has
much to do with her new husband and new job, her new attachments and new
achievements, though she would likely not have sought or found them without
taking Prozac. The drug itself did not make her happy; it merely enabled her to
do and experience the many things that make her happy. But now
imagine being Sally’s husband: Just to whom am I married? Would I love
Sally if she stopped taking Prozac and relapsed into timidity and hopelessness?
Would Sally love me? Would Sally be Sally?
With a drug like Ecstasy, the answers to such strange and
difficult questions—about the identity of the person taking such drugs and the
status of the positive feelings they induce—are more obvious, if no less
disquieting. People high on Ecstasy routinely profess their love for perfect
strangers. Imagine that a young party-goer, under the influence of the drug,
tells a young woman that he loves her and wants to marry her. Imagine also that
he means it, insofar as the feeling he now has is indistinguishable from what
he might one day feel when he truly falls in love with a woman. Should the fact
that his feelings are produced by the drug, rather than inspired by the woman,
matter? It should of course matter to her. His drug-based professions of
love cannot be taken seriously. Neither should a marriage proposal that owes
everything to his being “high.” But it should also matter to him, once
he awakens from the “alternative reality” induced by taking Ecstasy and
recovers the real identity that the drug temporarily erased.
The young man’s drug-induced “love” is not just
incomplete—an emotion unconnected with knowledge of and care for the beloved.
It is also unfounded, not based on anything—not even visible beauty—from which
such emotions normally grow. The young woman, were she to learn about his use
of Ecstasy, might readily agree: “He doesn’t really love me. It’s just the
drugs talking.” She might even say that the man is not really himself: “This
isn’t the real him; he isn’t in his right mind.” Insofar as his feelings are
attributable to Ecstasy, the young man’s feelings and words are, to speak
plainly, fake, indeed, doubly fake: they are neither true nor truly his.xxx
The drugs deceive him and induce him to behave in ways that could deceive
another.
In human affairs, we care a great deal about the difference
between “the real” and “the merely appearing.” We care about “living truly.” To
be sure, people for centuries have produced spurious feelings of all types with
alcohol and other agents. Yet although our society is generally tolerant of the
practice—alcohol, if not “harder” drugs—we do recognize the risks, limits, and
costs, not to mention the heightened possibilities of wrongdoing, connected
with “not being in one’s own right mind.” In fact, much of the disquiet often
voiced about mood-brightening drugs—even when appropriately used to treat
serious mental illness—clusters around this concern. Some patients fear
personality change, fear losing the “real me.” Some also worry about using
artificial means to change their psyches, a concern that springs ultimately
from their desire that feelings and personalities not be artificial and false
but genuine and true. Their worry, also widely shared, about having one’s
experiences of the world mediated by a drug is, at least in part, a worry about
having one’s real experience distorted. Even the expressed concern over “taking
the easy way out” may involve not so much an opposition to ease, but a concern
about distortion and self-deception.
With mood-brightening drugs like SSRIs, questions of
truthfulness and identity are indeed complicated. Unlike Ecstasy (a drug
regarded on multiple grounds as dangerous and declared illegal), SSRIs cannot
implant a groundless emotion, and they cannot instantly transform a soul.
Especially for the mentally ill, these drugs, far from distorting reality, may
enable patients to “get into their right mind” and to experience the
richness of life more fully and truthfully, sometimes for the first time. It
would thus be wrong and unfair to say that people whose lives are improved by
mood-brightening drugs live falsely or untruthfully, or that people taking
Prozac do not really love the husbands or wives they fell in love with while
taking their medication.
But while they do not live falsely, many of them do live
different lives than they would otherwise have lived, lives first made possible
because of the drug and often requiring its continued use to be sustained.
Though SSRIs do not instantly change the psyche, they can, gradually and over
time, induce a persisting background sense of well-being, even where well-being
itself is lacking. As a result, they can significantly change a person’s
temperament and therewith his personality, often markedly. According to the
striking testimony of some users, SSRIs allow them to “become themselves” again
or—strangely—to gain their true identity for the “first time.” This matter of
changed or transformed identity is, on its face, perplexing, with individuals
living lives and doing deeds they never did or could have done before taking
the drugs. And it remains for many a source of persisting disquiet.
Many people—perhaps all people, at some point—desire a
happier life than the one they have now. Dissatisfied with themselves, they
want to do better or feel better. In some cases, they opt for sharp and sudden
highs, for a brief “holiday from reality” made possible by drugs like alcohol,
heroin, or Ecstasy. In other cases, discontent spurs changed habits, new
pursuits, and better ways of living and behaving. In yet other cases, people
are and will be tempted to turn to mood-brightening drugs—SSRIs today, perhaps
more advanced drugs in the future—that might enable them more easily to do for
themselves the things they wish to do but cannot, or to feel the things they
wish to feel but do not, or to feel the things they once felt but can feel no
longer. While such drugs often make things better—they often help individuals
achieve some measure of the happiness they desire—taking such drugs may also
leave many of the same individuals wondering whether their newfound happiness
is fully their own—and in this sense, fully real. This concern persists
even when one becomes happy about genuinely happy things—like a new spouse or
new job. It is even more pertinent, and more disquieting, should one come to
feel happy for no good reason at all, or happy even when there remains much in
one’s life to be truly unhappy about.
2. Fitting Sensibilities and Human Attachments.
A central concern with mood-brightening drugs is that they
will estrange us emotionally from life as it really is, preventing us from
responding to events and experiences, whether good or bad, in a fitting way. Of
course, changing the way we respond to life’s happenings is a prime motive for
developing such drugs in the first place: to help individuals feel more joyful
about joyful things or less overwhelmed by their troubles and sorrows. And many
people, their neurobiological “equipment” defective, surely need psychopharmacological
assistance if they are to become able to respond fittingly to life’s many ups
and downs. But there is a danger that our new pharmacological remedies will
keep us “bright” or impassive in the face of things that ought to trouble,
sadden, outrage, or inspire us—that our medicated souls will stay flat no
matter what happens to us or around us.
Writing in his Confessions about the death of his
mother, St. Augustine provides a moving account of what it means to respond to
real life in a fitting way:
I closed her eyes; and there flowed a great sadness into my
heart, and it was passing into tears, when mine eyes at the same time, by the
violent control of my mind, sucked back the fountain dry, and woe was me in
such a struggle! . . . [I]n Thine ears, where none of them heard, did I blame
the softness of my feelings, and restrained the flow of my grief, which yielded
a little unto me; but the paroxysm returned again, though not so as to burst
forth into tears, nor to a change of countenance, though I knew what I
repressed in my heart. And as I was exceedingly annoyed that these human things
had such power over me, which in the due order and destiny of our natural
condition must of necessity come to pass, with a new sorrow I sorrowed for my
sorrow, and was wasted by a twofold sadness.34
At first blush, St. Augustine’s comments may strike a
modern reader as strange. He regarded his own grief, at least partially, as a failing,
believing that it betrayed too much concern for earthly things. But such grief
was, by his own admission, a “human thing,” a fitting response to the death of
the mother he loved dearly. What he felt was deep sadness at a deeply sad
event. If his response to his mother’s death had been hysterical unremitting
sorrow, we might think it excessive. And if he had been coldly indifferent, we
would wonder at his lack of humanity. The sadness he actually felt was the
humanly fitting response, the emotion called for and appropriate to the
circumstances. And yet, his sorrow, while fitting, also troubled him greatly.
Permit a somewhat outrageous thought experiment: might St.
Augustine’s physician, were such a drug available, have offered him a
mood-brightener? With it, St. Augustine might still have mourned, but with less
misery. He might have had to struggle less to “suck back the fountain dry,” or
to sorrow less for his own sorrowing. He might even have been less deflected
from his primary aspiration to attend to matters divine—if, that is, the drug
did not also flatten his longings. Would he, should he, have accepted such
pharmacological assistance?
If St. Augustine’s grief bothered him for theological
reasons, because of its excessive worldliness, the prospect of such grief
troubles many of our contemporaries for psychological reasons, either because
we want no such psychic burdens interfering with our worldly doings or because
we think we cannot endure them on our own. A desire for pharmacologic relief is
understandable. Some things, we fear, will simply hurt too much, if faced in
their unvarnished reality without somehow dulling the pain.xxxi
Yet especially in matters of love and death, such psychic relief may also
estrange us from the attachments that matter most. Seeking to “make the pain go
away,” or simply to ease it in the moment of its greatest sting, we risk giving
our departed loved one less significance than he or she deserves. Suffering “less
than we should,” we risk diminishing our appreciation of the depth of our love
and of the one whose absence now causes our pain.
This dilemma holds not only in matters of mourning. It
applies also to the pain of failing to achieve our goals or uphold our highest
principles, the pain of betraying or being betrayed by a friend, the pain of no
longer being able to do the things we once did with great ability and great
joy. Nothing hurts only if nothing matters. And while we rightly seek to reduce
the causes of gratuitous suffering, both physical and psychic, we do not want
to remove the capacity to suffer when suffering is called for.xxxii
It is true that in order to function in everyday life, one
needs some measure of detachment from the things that touch us most deeply. We
cannot and should not be filled to the emotional brim at every moment or wear
all our feelings on our sleeves. To feel things deeply and fittingly does not
require living without reticence or self-restraint. Yet by seeking psychic
detachment by means that pharmacologically insulate or remove us from the highs
and lows of real life, we may risk coming to love feebly or to care shallowly,
losing the fine texture of emotional and psychic life and weakening our
appreciation for the very human attachments that make life most meaningful.
3. What Sorrow Teaches, What Discontent Provokes.
The previous reflection casts a small doubt on the
unqualified goodness of the goal of a “happy soul.” “Feeling good” may not
always be good or good for us. Never to suffer loss may mean never to love
deeply; never to feel ashamed may mean that our standards for ourselves are too
low; never to be dissatisfied with ourselves may mean that we aspire to too
little. Even as we seek happiness, in other words, we must not overlook what
sorrow teaches and what discontent provokes—the intuitions, longings, and
hunger for improvement and understanding that make for a fuller and more
flourishing life.
There is, despite what the Romantics thought, no nobility
in having consumption (tuberculosis)—though there may be in how one copes with
it. So, too, there is no nobility in suffering from major depression or
crippling despair or even protracted grief following the death of a spouse or
child. In some cases, the very possibility of doing and living nobly and finely
may be crushed in ways that only mood-brightening drugs, properly used, can
help restore or repair. And clearly, one should not actively seek misery for
the lessons it might teach us, any more than one should seek to gain a fatal
disease in order to face it with courage or to relate better to those who
suffer from it.
But we cannot ignore the truth that life’s hardships often
make us better—more attuned to the hardships of others, more appreciative of
life’s everyday blessings, more aware of the things and the people that matter
most in our lives. Sadness in the recollection of a loss or a national tragedy
(for example, September 11) keeps alive and pays tribute to the blessings we
once enjoyed or still enjoy, gratuitously and vulnerably. Anxiety in the face
of a crucial meeting or big decision registers the importance of the
undertaking and prods us to rise to the occasion. Shame at our own
irresponsible or duplicitous conduct exhibits knowledge of proper conduct and
provides a spur to achieving it. These emotional stings not only reflect the
truth. If they do not crush us, they may make us better.
It seems paradoxical: sane people would never choose or
pray for sorrow, yet it is common to hear people say, after the fact, that
their darkest times were in some respects their finest hours and the source of
a better future. True, sorrows can often cripple or destroy. But sometimes, as
the philosopher Nicholas Wolterstorff writes in his Lament for a Son:
there emerges a radiance which elsewhere seldom appears: a
glow of courage, of love, of insight, of selflessness, of faith. In that
radiance we see best what humanity was meant to be. . . . In the valley of
suffering, despair and bitterness are brewed. But there also character is made.35
Sorrow, courageously confronted, can make us stronger,
wiser, and more compassionate.
To what extent might SSRIs, when used to reduce our
troubles and sorrows, endanger this aspect of affective life? Although they do
not prevent psychic pain, SSRIs may generally dull our capacity to feel it,
rendering us less capable of experiencing and learning from misfortune or
tragedy or empathizing with the miseries of others. If some virtues can only be
taught through very trying circumstances, those virtues might be lost or at
least less developed.
But it is not only the discontent thrust upon us by
external events or great misfortunes that can help to make us better. We can
benefit too from the discontent with our own deeds, actions, and character that
comes from honest self-examination. To be sure, many forms of self-loathing are
destructive or excessive, ranging from joyless perfectionism to suicidal
despair. But without some proper measure of self-discontent, there would be no
spur to self-improvement. If we never felt the emotional pangs of our own
shortcomings and limitations, we would never aspire to become better or wiser.
Just as physical pain prods us, say, to remove our hand from the hot stove,
psychic pain prods us, when it functions well, to improve those aspects of our
daily life (at work, at home, in the community) that are not “working well.”
Just as the pangs of hunger push us to nourish the body, so the pangs of
psychic hunger spur us to nourish the soul.
The motive force of passion is not confined to the negative
emotions. Positive emotions, too, when they are fitting and function well,
reinforce our attachment to what is good in our lives, encouraging us to
continue in the activities and human relationships that are fulfilling and to
preserve and enlarge the good things we seek and cherish. In a word, healthy
affect, negative as well as positive, is efficacious. It guides us to overall
well-being. Undermine that function—by means, say, of a drug that induces a
sense of well-being-no-matter-what in a person whose ordinary emotions are
functioning properly—and the cost is a life in which fitting feeling can no
longer guide or spur us toward living well.
In sum, a mood-brightening drug that always made us pleased
with ourselves no matter what we did—a drug that guaranteed our self-esteem,
even when such esteem is not warranted—might shrink our capacity for true human
flourishing.xxxiii
Possessed of full self-satisfaction, why would we be spurred to seek
improvement? Possessed of full peace of mind, why would we risk loss by giving
our heart to another or hazard disappointment by aspiring to something
difficult and noble? The example of “soma,” the drug in Aldous Huxley’s
fictional Brave New World, illustrates the debased value of a spurious,
drug-induced contentment.36
Soma—like cocaine, only without side effects or addiction—completely severs
feeling from living, inner sensation from all external relations, the feeling
of happiness from leading a good life. Rendered impotent in their aspirations,
the denizens of Huxley’s dystopia do not loathe their condition and do not
yearn for another, largely because they cannot loathe and cannot yearn. They
imagine themselves to be happy as they are, and thus never pursue a life that
would be more fully human, with the ups and downs that come from having
aspirations self-consciously chosen and ardently pursued.
SSRIs do not completely sever how one feels from how one
lives. On the contrary, in many therapeutic uses, they probably re-link feeling
and living, permitting passionate experience its proper role in fostering
further growth. But in certain uses and in certain people, these drugs may
fracture the relationship between passion and action, inducing calm, apathy,
and easy self-satisfaction where energy, engagement, and the desire for
self-improvement might be called for.
4. Medicalization of Self-Understanding.
Welcome though they are for those who really need them,
even the proper use of mood-brighteners to treat emotional disorders is not
without hazard. Precisely because of the effectiveness of the medication to
alter mood and self-esteem, there may well be a tendency to redefine, in
medical and biological terms, what are currently considered normal emotions,
moods, and temperaments. Because the psychic pains of mental illness are akin
or sufficiently similar to the psychic pains of ordinary life, there will be a
natural tendency to regard ordinary affective life through the lens first
polished for viewing mental disorders.xxxiv
Such medicalized understanding might well make suffering easier to cope with.
For example, a person who attributes his discontent or sadness to sickness may
spare himself difficult self-examination and self-recrimination, as well as
arduous attempts to change the way he lives. He can take mood-brighteners
without guilt or without any sense that he is missing something. But this
benefit, if it is that, may well come at considerable cost. For one reconceives
sadness as sickness only by emptying it of psychic or spiritual significance
and turning it into a mere thing of the body. Not only is the soul seen as
dissolved into the body, but the body itself is seen as dissolved into genes
and neurochemicals. Ardent desire is reduced to an elevated peptide
concentration in the hypothalamus, righteous indignation is reduced to an
elevated serotonin level in the temporal lobe. In the limit, happiness itself,
along with misery, can be reconceived as a matter of neurons and
neurotransmitter levels. No longer a spiritual achievement or the fruit of a
life well-lived, it can come to be seen as the gift of either natural good
fortune or biotechnical manipulation. The medicalization of psychic pain,
however necessary as a path to providing much needed relief for the sick,
indicates (whether intended or not) a great advance for biological reductionism
against the citadel of mind and soul, a march that knows no natural stopping
place, and that at each point along the advance threatens to reduce further the
dignity of our inner life—or at least our self-understanding of it.
Our concern regarding such a transformation is not merely
of theoretic or conceptual importance. It is also practical, affecting how
doctors treat patients and the problems they bring to the doctor’s door. Thanks
to the efficacy of mood brightening agents, and of psychotropic drugs more
generally, there may well be a temptation to redefine and to treat what
are currently considered normal emotions, moods, and temperaments on the model
of mental illness, and mental illness as a matter purely of bodily—ultimately,
of molecular—character and causation. Should this occur, there will be large
difficulties in assigning moral responsibility for any improper (or, for that
matter, admirable) behavior, not only in matters criminal but in all
interpersonal relations.
Are normal emotions or normal problems of living today
being “diagnosed” or regarded in the way we regard mental illness? Is
medicalization actually taking place, in practice as well as in thought? It is
hard to say, and careful social science research would be needed before an
answer could be hazarded with confidence. And a positive answer, in some
cases, need not be cause for concern. It is possible that temperaments we
once saw as typically human—habitual mild melancholy, for example, or shyness, or
alienation, or inhibition—will be shown indisputably to result from definite
neurochemical abnormalities. Epilepsy was once thought to show demonic
possession (“The Sacred Disease”), and manic depression was thought to reveal
bad character. Both diseases were stigmatized and treated ineffectively. Now,
thankfully, both epilepsy and bipolar disorder have been entirely medicalized,
both in idea and in practice. Medicalizing the problems of living, and using
drugs to brighten a healthy mood, may have serious human costs, but so does
refusing to use beneficial medication when one is sick and treating problems of
health as problems of character. Good medicine and sound ethics thus have the
same interest: effectively treating the sick in light of a sound conception of
human health, without treating as illness every troubled state of soul.
Many psychiatrists, keenly aware of the problem, already
understand their mission in these terms. A leading book in the field introduces
the subject of depression by explaining that, of the patients who turn to a
doctor because they are feeling downhearted, “the majority . . . will be facing
a serious life situation,” while some “will be suffering not from some
responsive mood but from a fixed depressive state,” which then “must be
recognized for what it is, major depression.”37
The DSM-IV requires for a diagnosis of major depression or dysthymia that “[t]he
symptoms cause clinically significant distress or impairment in social,
occupational, or other important areas of functioning.”38
If doctors maintain high diagnostic standards, treating with mood-brightening
drugs only those patients who have an illness, are sliding into one, or whose
emotional troubles are so urgent as to make claims on the duty to save, the
worst excesses of using mood-brighteners can perhaps be avoided or reduced.
Yet we should not be complacent. Many forces and incentives
are pushing us in the opposite direction. As already noted, the arrival of
efficacious mood-brightening (and other psychotropic) drugs invites enlargement
of the domain of illness and further reductionist thinking about its cause.
Doctors are the gatekeepers to drugs, drugs are prescribed (and their costs
reimbursed) only for diagnosed illnesses, and the growing demand for drugs—a
demand in part deliberately created by their manufacturers in direct
advertising to consumers—exerts great pressure for the expansion of diagnostic
categories. Even were the medical profession interested in developing a sound
and limited concept of health, a workable account is hard to come by, and,
truth to tell, the search for it is rarely undertaken. Especially as health
comes to be regarded less as the absence of disease but as some positive state
of well-being, ever open-ended and unlimited in its boundaries, the incentive
increases to medicalize not only health but all human activities, psychic and
social.xxxv
One need not philosophically embrace
the World Health Organization’s notorious definition of health—as “complete
physical, mental, and social well-being”—to contribute in practice to making
human happiness a growing part of the doctor’s business, ever more open to
pharmacological assistance.
5. The Roots of Human Flourishing.
As we noted at the start of this chapter, the nature of
human happiness is a contested matter, not only between different cultures but
within any one culture. Western thought boasts many distinguished accounts of
how emotions and feelings are, and should be, involved with human flourishing
or human happiness. An important issue in dispute is the connection between “feeling
pleasure” and “being happy,” a question advertised in the ambiguities of the
word “happiness,” perched as it is between “pleasure” and “flourishing,”
between “feeling good” and “living well.” A most prominent ethical outlook,
utilitarianism, seeks the greatest happiness for the greatest number, with
happiness often measured solely by self-reported pleasure or contentment. On
such a view, mood-brightening technology might be regarded as an unequivocal good,
a direct contribution to greater human happiness, whose only cost would be any
pleasure it might prevent or obstruct, say, through side effects or addiction.
A very different picture of what it means to flourish
emotionally emerges from the ethical analysis presented above. Perpetual bliss
would not be the emotional ideal (at least in the world we inhabit), because
emotional flourishing of human beings in this world requires that feelings jibe
with the truth of things, both as effect and as cause. As response, affect is
at its best when it exhibits certain cognitive and aesthetic virtues like
measure and proportion; the criterion is that it be fitting. As motive, affect
should lead a person to seek out a good life or to preserve the one he has; the
criterion is that it be efficacious in service to the good to which the emotion
points, whether positively or negatively. When affect is a healthy part of a
psychic whole, it serves not the limited purpose of pleasure alone, but serves
and helps constitute overall human flourishing.
Taking an additional step, we suggest that, under
conditions of psychic health, the moods of the mind and the experienced
pleasures, both of soul and body, are neither primary nor independent aspects
of our lives. They are rather derived from and tied to the things we do and
encounter: the people we meet, love, and lose, and the children we rear; the
activities we pursue and the successes and failures that we encounter; the
thoughts we have and the judgments we make; the beauty we admire and the evils
we abhor. Moreover, because human activities and experiences differ greatly
among themselves, so, too, do the attendant pleasures and pains differ in kind
and in quality. Whatever we may assert in speech about the supremacy and homogeneity
of pleasure or satisfaction, we care in fact primarily about activity and
experience, and we care also about the quality of the pleasure and
satisfaction. We do not really want the pleasure without the activity: we do
not want the pleasure of playing baseball without playing baseball, the
pleasure of listening to music without the music, the satisfaction of having
learned something without knowing anything. Pleasure follows in the wake of the
activity and, as it were, lights it up into consciousness. But without the
activity there is and can be no happiness. We embrace neither suffering nor
self-denial by suggesting that disconnected pleasure (or contentment or
self-esteem or brightness of mood) produced from out of a bottle is but a poor
substitute for happiness.
Where does this leave us regarding the relation between
mood-brighteners and happy souls? We human beings share with all higher animals
a predilection for feelings of comfort and pleasure. But our uniquely human
capacity is to recognize that all the pokings, proddings, and temptings of
feeling are like arrows that point us to lives of meaning and purpose. And
recognizing the direction of our aspiration, we also find in ourselves the
eminently human capacity to desire and direct its aim. There have always been
those who, seeing how intense and how woven into our various enterprises is the
desire for pleasure, think its satisfaction the whole point of human life. If
that were true, the potential appeal of mood-brightening drugs would appear limitless.
But if, as we have suggested, it is not true, then to put
mood-brightening technology to its best human use is to use it sparingly,
medically, to help those who cannot do so unassisted to attain the capacity for
securing fitting relationships between their feelings, their causes, and their
effects. It is to help them achieve an appropriate relationship between their
circumstances, inner life, and possibilities for action, so that they are able
to feel joy at joyous events and sadness at sad ones, to marvel at the world’s
wonders, resist cruelties, and all the while strive to develop their talents,
honor their obligations, and cherish their friendships and loves. For none of
us lives humanly by the feeling of untroubled ease alone.
6. The Happy Self and the Good Society.
So far, we have focused largely on the meaning of using
mood-brightening drugs for the individual, and the danger of gaining peace of
mind at the cost of living less truly or not being oneself. But individuals do
not pursue happiness alone as solitary beings, nor is the search for individual
well-being, narrowly understood, the sole or even central purpose of our lives.
The individual depends on others to live a full and flourishing human life—on
farmers to feed him, teachers to guide him, soldiers to protect him, family and
friends to stand with him. His very identity is embedded in a web of
overlapping communities—family, neighborhood, institutions of work and worship,
nation. And these communities often need individuals to put the good of the
whole before their own inner (or inward-looking) search for happiness. If human
beings were merely self-absorbed, all good and lasting things would wither.
At the same time, we also cannot ignore the great
achievement of liberal society in its concern for the dignity of the individual
person—for seeing individuals not simply as useful and expendable means to
society’s ends, but as ends in themselves. Their individual well-being must be
regarded and protected, not only against oppressive government or religious
authority, but also against the tyranny of the majority and the ruling opinions
and conventions of society.
The availability and use of mood-brightening drugs creates
(and reflects) potential dangers in these two corresponding directions. The
first danger is that individuals will become so preoccupied with their own
state of mind that they remove themselves increasingly from active
participation in civic life, discarding those attachments without which they
cannot achieve the happiness they seek and without which the community cannot
survive and flourish. The second danger is that social goals or
expectations—the external pressure to be productive, to gain status and
recognition, to get ahead—will produce a “mood-brightened society,” where
pharmacological interventions in our psyches become normal or expected for
students, employees, and ultimately everyone. Put simply, the first danger
involves the solipsistic self, worried only about the state of his feelings,
who uses psychopharmacology to ensure a flat and shallow self-regarding psychic
pleasure. The second danger involves the slavish self, whose worth is measured
only in the eyes of others or according to his success in the rat race, and who
takes mood-brightening (or other) drugs to assert himself or to increase his
chances of meeting society’s demands. Neither alternative bodes well for a free
society.
Needless to say, one is hesitant to fault doctors and
individuals who use mood-brightening drugs in search of relief from melancholy
or malaise in cases where indications of serious depression are unclear. The
decision to medicate in such cases, often difficult and full of ambivalence, is
usually best made by patients and physicians in private. But we also cannot
ignore the potential social consequences if self-medication of the soul, freely
and individually chosen, were to become the social norm. Nor can we ignore the
present culture in which these individual choices are made: a culture that
prizes self-esteem, self-fulfillment, and self-advancement, and that
increasingly looks to modern medicine to heal the troubled self. Indeed, new
drugs for the psyche, new direct-to-consumer advertisements promising greater
happiness through pharmacology, an expanding number of mental illnesses with
ever broader criteria of diagnosis—this potent brew may already be creating new
anxieties about mental health and new desires for mood-brightening drugs where
neither existed before. These newly created desires, and the self-understanding
that accompanies them, can transform the souls of a society even more
profoundly than the drugs themselves.
Perhaps a remedy for our psychic troubles lies in the
rediscovery of obligations and purposes outside the self—a turn outward rather
than inward, a turn from the healthy mind to the good society. And perhaps the
most promising route to real happiness is to live a fully engaged life, as
teachers and parents, soldiers and statesmen, doctors and volunteers—in short,
to follow the vocations of life that involve not the self alone, but the ties
that bind and that ultimately give the individual’s identity its true shape. To
be sure, there are many people whose deep psychic distress precludes meeting
obligations and forming close relationships, and for whom the proper use of
mood-brighteners is the blessed gift that can restore to them the chance for a
full and flourishing life. But there is also a danger that such drugs, suitably
improved and refined, may one day offer us peace of mind not only without side
effects but also without exertion or interest in human attachments—a peace of
mind that might rival friends, family, and country for our deepest devotion.
IV. Conclusion
The promise and the peril of memory-blunting and
mood-brightening drugs may prove to be quite profound. The awesome powers
modern science has placed in our hands to control the external world
increasingly enable us to control our inner experience, indeed to sever the
link between subjective experience and our actions in the world. Not only can
we produce an enormous range of things that make us happy—including stronger
bodies, smarter minds, and stronger and smarter children—but increasingly we
can produce through drugs the subjective experience of contentment and
well-being in the absence of the goods that normally engender them. In some
cases—as with traumatic memories or a pervasive and crippling sense of anxiety
and despair—the new drugs can help return a person to the world and enable him
to take responsibility for his life. But in many other cases, the growing power
to manage our mental lives pharmacologically threatens our happiness by
estranging us not only from the world but also from the sentiments, passions,
and qualities of mind and character that enable us to live in it well.
Living well in the world has always meant striving for
physical pleasure, wealth, honor, recognition, friendship, love, understanding,
and spiritual fulfillment. And no small part of the challenge has been to
reconcile the conflicting demands of these abiding human goods. In responding
to the challenge, it has always been advantageous to be strong of body and
sound of mind, and it has always been a pleasure to move freely under one’s own
power and to understand accurately the ways of the world. Nearly all the goods
we seek involve living well with others, so some knowledge of the human heart
is indispensable to our happiness. Since friendship and love, the goods for
which we often long most, indissolubly link the happiness of others to our
happiness, we also have a keen interest in that sympathetic understanding that
allows us to figure out both our own wants, needs, and desires and those of our
friends and family members. In other words, happiness today, as always,
consists in the activity of the well-functioning and self-aware soul.
Memory- and mood-altering drugs pose a fundamental danger
to our pursuit of happiness. In the process of satisfying our genuine desires
for peace of mind, a cheerful outlook, unclouded self-esteem, and intense
pleasure, they may impair our capacity to satisfy the desires that by nature
make us happiest. The fashioning of a memory that does not reflect how we have
shaped and been shaped by experience threatens to bestow upon us satisfactions
that are not truly our own. And the creating of calmer moods and moments of
heightened pleasure or self-satisfaction that bear no relation to our actual
undertakings threatens to erode our sentiments, passions, and virtues. What is
to be particularly feared about the increasingly common and casual use of mind-altering
drugs, then, is not that they will induce us to dwell on happiness at the
expense of other human goods, but that they will seduce us into resting content
with a shallow and factitious happiness.
It is no great surprise that it is our freedom-loving,
technology-fancying, and happiness-chasing society that is bringing these wares
to market. Yet these drugs also pose a fundamental danger to a society based on
the individual’s right to the pursuit of happiness. A society whose citizens
can obtain tranquility on demand and enjoy no-fault ecstasy is a society whose
citizens are bound to be less prepared to perform the responsibilities incident
to citizenship in a free country. Wise policy is not derived from a formula.
Laws are not self-enacting. Emergencies, resulting both from acts of nature and
from acts of human recklessness and cruelty, will happen. But who will judge
wisely, who will act honorably, who will rise to the occasion should drugs
increasingly estrange us from the satisfactions connected to acting wisely and
well? Who will take seriously even the everyday duties to kith and kin in a
world that esteems—and uses medicine to produce—self-satisfied egos, looking
out only for Number One?
The remedy for the new individual and social dangers to
which our freedom exposes us must be consistent with our right to “the pursuit
of happiness.” And so it is. For the remedy consists in organizing our lives
around happiness rightly understood, and our freedom gives us the opportunity
to acquire that understanding and act upon it. In the end, it is happiness
understood as complete and comprehensive well-being, or happiness of the soul,
that we seek. And the happiness of the soul is inseparable from the pleasure
that comes from perfecting our natures and living fruitfully with our families,
friends, and fellow citizens.
No doubt the amazing new world of biotechnology has an
enormous role to play in our soul’s aspiration for happiness. Whether it will
further or frustrate that aspiration depends in no small measure on our ability
to clarify happiness’s character and content. It depends especially on our
willingness, both as individuals and as a society, not to settle for a shallow
and shrunken imitation.
Footnotes
i. “Pursuit” is here properly ambiguous, encompassing both the
quest to find happiness and the enjoyment of happiness once found (as in “my
favorite pursuits”).
ii. We note at the outset of this discussion that some people
do not regard happiness as the supreme goal, preferring instead to place
righteousness, duty, virtuous and creative activity, or holiness and serving
God at the peak of human aspiration. Whether or not this remains a disagreement
depends finally on whether happiness, if understood as human fulfillment,
embraces these other goals as well, or whether it is distinct from them.
iii. John Locke, one source of our present views of happiness,
wrote that the quest for happiness is, in fact, nothing more than an effort to
alleviate “the uneasiness a man is at present under.” (Essay Concerning
Human Understanding [1690], Chapter XXI, “Of Power,” §31.)
iv. Once again, whether we in fact accept these invitations to
change our self-understanding and whether, if we do, the baneful consequences
(for the fitness and truthfulness of our emotional lives) will in fact follow
are empirical questions, to be investigated in future research, but not
therefore to be banished from current reflection.
v. At the same time, it is important to note that “stored memories”
do not remain static. Every time we recall a memory, what gets stored after
such acts of recollection is a different memory, altered on account of how we,
in recollecting it, have “received” and reacted to it. Once encoded, memories
can be altered by recall.
vi. We also know that individuals “naturally” edit their memory of
traumatic or significant events—both giving new meaning to the past in light of
new experiences and in some cases distorting the past to make it more bearable.
The question before us is how or whether new biotechnical interventions alter
this inborn capacity to refine, reshape, and edit the way we remember the past.
vii. A few recent findings were noted in Chapter Four, “Ageless
Bodies.”
viii. Of course, this is not to say that the use of “memory-enhancers”
would be a simple matter, ethically or socially. Such drugs, if they became
available, would likely have many “beyond therapy” uses; they would raise
questions about the meaning of enhancing cognitive performance
pharmacologically and the meaning of “normal” memory decline that accompanies
aging, both matters we discuss or at least touch on in other parts of this
report.
ix. Schacter finds that our memory commits the following “seven
sins”: transience, absent-mindedness, blocking, misattribution, suggestibility,
bias, and persistence. While each of these failings can sometimes be a
nuisance, they are also, he argues, necessary for our survival. See Schacter,
D., Presentation at the October 2002 meeting of the President’s Council on
Bioethics, Washington, D.C. Transcript available on the Council’s website at
www.bioethics.gov; also Schacter, D., The Seven Sins of Memory: How the Mind Forgets and
Remembers, New York: Houghton Mifflin, 2001, p. 4 ff.
x. An individual with “retrograde amnesia” suffers from a
sudden loss, either partial or total, of his own memory of the past. His
personal past is inaccessible to him; it remains known and remembered only (and
necessarily only in part) by others. Though he can learn new things, he remains
a stranger to his world, thrown into a life and human relationships that he has
no memory of forming. In contrast, an individual with “anterograde amnesia”
suffers from the inability to remember new things, new events, or new
experiences. The past remains intact as memory, but he is unable to move beyond
it. Although the sufferer remains himself, he remains psychically fixed in
time, with mind and body, self-consciousness and reality, alienated from one
another.
xi. “The utility of all the passions consists only in their
fortifying and prolonging in the soul those thoughts which it is good for it to
conserve and which otherwise may be easily effaced; as also all the harm they
can cause consists in their fortifying and conserving these thoughts more than
is needed, or in fortifying and conserving others which ought not to be fixed
there.” (Descartes, The Passions of the Soul [1649], § 74.)
xii. As crucial as animal research is to providing insight about
the workings of human memory, we must also keep in mind the limits of the
comparison. The character of human memory is so distinct, involving experiences
so foreign to other animals, that shared systems of the brain may have very
different functional and experiential meanings, and crucial subtleties may be
lost in seeing only the broad neurological similarities. The hazard of
extrapolating too much from other animals to human beings is always present in
research—but perhaps especially in the case of memory and other
psychological-moral experiences that are singularly human.
xiii. Beta-blockers—more precisely, beta-adrenergic receptor
antagonists—such as propranolol were originally developed in the 1960s (and
today are still chiefly used) for the prevention and treatment of heart disease
and hypertension.
xiv. Long-time and sizable clinical experience with beta-blockers
in treatment of heart disease and hypertension has not revealed memory defects
or personality change to be major side effects. Yet one might not expect to see
their memory-blunting power except in the face of the huge adrenaline
outpourings associated with frightening and horrifying experiences.
xv. These symptoms are observed especially among combat veterans;
indeed, PTSD is the modern name for what used to be called “shell shock” or “combat
neurosis.” Among veterans, PTSD is frequently associated with recurrent
nightmares, substance abuse, and delusional outbursts of violence. There is
controversy about the prevalence of PTSD, with some studies finding that up to
8 percent of adult Americans have suffered the disorder, as well as a third of
all veterans of the Vietnam War. See Kessler, R. C., et al., “Post-Traumatic
Stress Disorder in the National Comorbidity Survey,” Archives of General
Psychiatry 52(12): 1048-1060, 1995; Kulka, R. A., et al., Trauma and the
Vietnam War Generation: Report of Findings from the National Vietnam Veterans
Readjustment Study, New York: Brunner/Mazel, 1990.
xvi. There is already ongoing controversy about excessive
diagnosis of PTSD. Many psychotherapists believe that a patient’s psychic
troubles are generally based on some earlier (now repressed) traumatic
experience which must be unearthed and dealt with if relief is to be found.
True PTSD is, however, generally transient, and the search for treatment is
directed against the symptoms of its initial (worst) phase—the sleeplessness,
the nightmares, the excessive jitteriness.
xvii. Of course, many Holocaust survivors managed, without
pharmacological assistance, to live fulfilling lives while never forgetting
what they lived through. At the same time, many survivors would almost
certainly have benefited from pharmacological treatment.
xviii. The term harkens back to the time when these dispositions
were thought to be the result of the temper, or balance, of the body’s
so-called “four humors”: blood, phlegm, bile, and black bile. As a result of
insufficiently tempered mixtures, so the theory had it, persons with an
unbalanced excess of one or another of the humors would be of sanguine,
phlegmatic, choleric, or melancholic temperaments. It has been noted that
current scientific efforts to tie temperaments to various imbalances in
neurotransmitter levels in the brain may be regarded as a modern scientific “revival”
of the idea that “humoral tempering” is central to determining our emotional
outlooks.
xvix. The difficulty in describing the effects of psychotropic
agents is very likely inherent in the difficulty in describing the psychic
phenomena themselves. Regarding our “inner experience,” we are often stuck with
metaphors—”higher,” “brighter,” “depressed”—including the spatial metaphor of “inwardness”
itself. We return to this topic when we treat the effects of some of the drugs
now most commonly in use.
xx. Effexor also inhibits norepinephrine and is sometimes
referred to as an SNRI (serotonin-norepinephrine reuptake inhibitor). In this
chapter, for convenience, it can be assumed under the heading of SSRI. Some
other agents, such as the aminoketone Wellbutrin, are used in ways similar to
SSRIs; the analysis that follows may also apply or apply partially to them.
xxi. There is some evidence that major depression may be
associated with reduced volume in the hippocampus, perhaps reflecting a loss of
neurons in that part of the brain; furthermore, very recent studies suggest
that treatment with SSRIs (as well as other antidepressants) leads to
significant neurogenesis (new growth of neuron cells) in the hippocampus. It
is, however, far too early to say whether hippocampal atrophy is a major cause
of depression, or whether the antidepressant efficacy of SSRIs and other drugs
is in fact mediated by stimulation of neurogenesis. See Sheline, Y. I., et al.,
“Hippocampal atrophy in recurrent major depression,” Proceedings of the
National Academy of Sciences, 93: 3908-3913, 1996; Santarelli, L., et al., “Requirement
of Hippocampal Neurogenesis for the Behavioral Effects of Antidepressants,” Science,
301: 805-809, 2003.
xxii. The Diagnostic and Statistical Manual of Mental
Disorders, Fourth Edition (DSM-IV) is the psychiatric community’s
authoritative guide to diagnosis. Its chief and stated purpose is to “provide a
helpful guide to clinical practice” (p. xxiii).
xxiii. This line of variation has been differently described as
the neuroticism-stability dimension, the unstable-stable dimension, or the
strong-weak dimension, of human temperament. But as the names suggest, part of
the model’s clinical importance is in explaining emotional vulnerability: the
more intense one’s moods and emotions, the more likely one is to fall into a
variety of behaviors and states of mind that are troubling.
xxiv. A calmer disposition might then permit more fitting
emotional responses to particular experiences. Arguably, SSRIs might also
shrink the range of emotional responses, raising the floor but lowering the
ceiling.
xxv. MDMA functions differently from SSRIs: rather than inhibiting
serotonin reuptake, it increases serotonin production, causing massive dumps of
serotonin into the synapses. Yet to the receiving neuron, more serotonin is
available either way. Whether the difference between SSRIs and MDMA is one of
degree or of kind, and what the example of one means for the other, is not
clear.
xxvi. For example, lobsters show increased serotonin production
when nearing food sources. Primates’ levels of serotonin correlate with their
position in the social hierarchy. (Peter Kramer, presentation at the September
2002 meeting of the President’s Council on Bioethics, Washington, D.C.
Transcript available on the Council’s web site at www.bioethics.gov.) The
examples are both suggestive and perplexing. Lobsters seem unlikely to have
emotions or moods of a fine-grained sort. Yet primates of high social status
show a wide range of emotions and moods (presumably while enjoying high
serotonin levels). Perhaps serotonin is involved with something more basic than
emotion and mood, something less specific yet still registering the difference
between positive and negative.
xxvii. We are not unaware of the strangeness of the claim that
such a hypothetical identity, previously hidden but newly released, would be
identical to one that would have been formed in a life differently lived.
xxviii. “This research is pushing psychiatry toward the treatment
of ever more minor levels of mood disruption; there is, in other words, an
empirical rationale for expanding the range of psychiatric diagnosis. It may be
appropriate to medicate patients whose level of depression is “subsyndromal”—certainly
a melancholic person may be a fit candidate for that other mental health
technology, psychotherapy—but I would say that an honest labeling of this use
of antidepressants would deem it an attempt, through pharmacology, to replace a
normal if unrewarded personality style with another normal style that is more
comfortable or better socially rewarded.” (Kramer, P., Listening to Prozac,
Second Edition, New York: Penguin, 1997, p.322.)
xxix. Consider the analogy of “treating” the anxiety and
disproportionate urgency (and associated danger) of adolescent sexuality by
extinguishing it at its biochemical source (note that in some patients Prozac
will diminish libido). This fundamental biological drive, and its attendant
discontent, is inextricably related to the larger longings of romantic love and
in turn to some of life’s highest aspirations and achievements.
xxx. The subject of true love and love potions is, of course, a
familiar theme of great literature, from the myth of Tristan and Isolde to
Shakespeare’s A Midsummer Night’s Dream. These writings are interested
in the degree to which eros itself is like divine, demonic, or “magical”
possession. Are people who fall in love in their own “right minds”?
xxxi. Many a person has drowned his sorrows in alcohol, though it
should be added that—unlike with the use of mood-brighteners—sorrow returns the
morning after, often made worse by a hangover. And chronic drunkenness brings
its own miseries and sorrows.
xxxii. This point about psychic pain and psychic fitness exactly
parallels the situation regarding bodily pain and fitness. We try to prevent or
treat gratuitous pain, but we recognize the life-saving and fitness-preserving
virtues of the capacity to feel pain. Full analgesia is deadly.
xxxiii. The cultivation and corruptions of a spurious self-esteem
are, of course, possible without using drugs. Examples abound in our current
cultural climate.
xxxiv. The same thing happened with psychoanalysis, where a theory
devised to explain neurosis became the ruling explanation of all psychic life,
abnormal and normal.
xxxv. Proposals are now circulating among psychiatrists to define
a new “relational disorder” to cover people with serious marital difficulties,
including spousal abuse.
Endnotes
1. Aristotle, Nicomachean Ethics, 1095a17-20.
2. Borges, J. L., “Funes the Memorious,” in Ficciones, John Sturrock, ed. (original publication 1942; English transl., Grove Press, 1962; rpt. by Alfred A. Knopf/Everyman, 1993), pp. 83-91; Luria, A. R., The Mind of a Mnemonist: A little book about a vast memory (Solotaroff, L., trans.), New York: Basic Books, 1968.
3. On this research see LeDoux, J. E., “Emotion, Memory, and the
Brain,” Scientific
American, 270: 32-39, 1994; McGaugh, J., “Emotional Activation,
Neuromodulatory Systems and Memory,” in Memory Distortion: How Minds, Brains, and Societies
Reconstruct the Past, edited by D. Schacter, et al., pp. 255-273,
1995; and McGaugh, J., “Memory consolidation and the amygdala: a system
perspective,” Trends
in Neuroscience, 25(9): 456-461, 2002.
4. Cahill, L., et al., “Beta-Adrenergic activation and memory for
emotional events,”Nature,
371: 702-704, 1994.
5. Pitman, R. K., et al., “Pilot Study of Secondary Prevention of
Posttraumatic Stress Disorder with Propranolol,”Biological Psychiatry, 51: 189-192, 2002.
6. See, for example, Goodman, E., “Matter Over Mind?,” Washington
Post, November 16, 2002, and Baard, E., “The Guilt-Free Soldier,” Village
Voice, 28 January 2003. It is interesting to note the dual appeal of such
drugs to both the traumatized victim seeking escape from the horror of his or
her experience and the traumatizing assailant looking to escape the
inconvenience of his guilty memory.
7. There is no definitive diagnostic criterion for PTSD, but the
core symptoms are thought to include persistent re-experiencing of the
traumatic event, avoidance of associated stimuli, and hyperarousal. See Diagnostic
and Statistical Manual of Mental Disorders, Fourth Edition, text revision,
Washington, D.C.: American Psychiatric Association, 2000, pp. 463-486.
8. Schacter, D., The
Seven Sins of Memory: How the Mind Forgets and Remembers, New York:
Houghton Mifflin, 2001, p. 183.
9. For a discussion of memory-altering drugs and the meaning of “bearing
witness,” see the essay by Cohen, E., “Our Psychotropic Memory,” SEED,
no. 8, Fall 2003, p.42.
10. Austen, Jane, Mansfield Park (1814), Ch. 22.
11. See http://abcnews.go.com/onair/WorldNewsTonight/poll000410.html.
12. Kramer, P., Listening to Prozac, New York: Penguin,
1997, p. 66. The point is thematic throughout the book; see also, for example,
pp. 46, 89, 125-127, and 320-322. See also Braun, S., The Science of
Happiness: Unlocking the Mysteries of Mood, New York: John Wiley &
Sons, 2000, pp. 8-9 and 161-181, and Barondes, S., Better Than Prozac: The
Future of Psychiatric Drugs, Oxford: Oxford University Press, 2003.
Relatively little academic research, as opposed to clinical observation, has
been done on this issue. What has been done supports the idea that SSRIs affect
the mood of people without severe illness, ranging from mild depression to
normalcy. See Dunlop, S. R., et al., “Pattern Analysis Shows Beneficial Effect
of Fluoxetine Treatment in Mild Depression,” Psychopharmacology Bulletin,
26: 173-180, 1990; Knutson, B., et al., “Selective Alteration of Personality
and Social Behavior by Serotonergic Intervention,” American Journal of
Psychiatry 155: 373-379, 1998; Liotti, M., et al., “Differential
Limbic-Cortical Correlates of Sadness and Anxiety in Healthy Subjects:
Implications for Affective Disorders,” Biological Psychiatry, 48: 30-42,
2000.
13. Dozens of books aimed at a general audience about
mood-brighteners, in particular the SSRI Prozac, have been published in the last
decade alone (some are listed in endnote 12). Popular articles abound in
publications ranging from the New York Times to Newsweek to Glamour
(Slater, L., “Prozac Mother and Child,” New York Times Magazine, 17
October 1999, pp. 15-17; Gates, D., “The Case of Dr. Strangedrug,” Newsweek,
19 June 1993; Fried, S., “Addicted to Antidepressants? The Controversy Over a
Pill Millions of Us Are Taking,” Glamour, April 2003, pp. 178-180, 262).
Television programs have also covered the matter, including “Nightline,” “Geraldo,”
the “Today” show, “60 Minutes,” “Donahue,” “Larry King,” “Eye on America,” and “Prime
Time Live.” The tremendous coverage, while highly varied in quality, indicates
the degree to which drugs that touch on such deep and universal human
aspirations provoke interest.
14. For one, among many, moving accounts of major depressive
illness and its associated risks, including risk of suicide, see Rosenberg, L.,
“Brainsick: A Physician’s Journey to the Brink,” Cerebrum, 4: 43-60,
2002.
15. Kramer, P., Listening to Prozac, pp. 15-16, 44-46,
321-322. This point is one of Kramer’s principal themes. See also Barondes, S.,
Better Than Prozac, op. cit.
16. The National Institute of Mental Health, The Numbers
Count: Mental Disorders in America, Washington, D.C.: NIH Publication No.
01-4584, 2003, p. 1; Sapolsky, R., “Will We Still Be Sad Fifty Years from Now?”
in Brockman, J., The Next Fifty Years: Science in the First Half of the
Twenty-First Century, New York: Vintage, 2002, p. 106; Nestler, E.J., et
al., “Neurobiology of Depression,” Neuron, 34: 13-25, p. 13, 2002.
17. Klerman, G., et al., “Increasing rates of depression,” Journal
of the American Medical Association, 261(15): 2229-2235, 1989; see also
Sapolsky, R., “Will We Still Be Sad Fifty Years from Now?” op. cit., pp.
106-107.
18. See the references cited in endnotes 12 and 16.
19. The National Institute of Mental Health, Medications,
Washington, DC: NIH Publication No. 02-3929, 2002, p. 20; Nestler, “Neurobiology
of Depression,” op. cit., p. 15.
20. Glader, P., “From the Maker of Effexor: Campus Forums on
Depression,” Wall Street Journal, 10 October 2002, p. B1. Very little
definitive information on the prevalence of mood-brighteners among college
students is available. One survey suggests that only slightly over 4 percent of
students are currently taking mood-brighteners (American College Health
Association, National College Health Assessment: Reference Group Executive
Summary Spring 2002, Baltimore: American College Health Association, 2002).
But this assessment does not speak to how many have taken them, and it
contradicts the impressions of many college officials.
21. Nestler, “Neurobiology of Depression,” op. cit.
22. Diagnostic and Statistical Manual of Mental Disorders, op.
cit., pp. 345-428.
23. Nestler, op. cit.; Healy, D., The Antidepressant
Era, Cambridge: Harvard, p. 174, 1997.
24. Nestler, “Neurobiology of Depression,” op. cit., p. 13.
Braun, The Science of Happiness, op. cit., pp. 17-18.
25. See Listening to Prozac, op. cit.; The
Science of Happiness, op. cit., p. 12 and pp. 161-181; Better Than
Prozac, op. cit.
26. For a discussion of both this aspect of temperament and the
capacity of SSRIs to affect it, see McHugh, P., et al., The Perspectives of
Psychiatry, Baltimore: Johns Hopkins, 1998, pp. 132-135.
27. For a report of the experience of taking MDMA, see Klam, M., “Experiencing
Ecstasy,” The New York Times Magazine, 21 January 2001.
28. A related line of thought has been developed by Michael
McGuire. See Kramer, Listening to Prozac, 169.
29. Listening to Prozac, pp. 144-148, 162, 177, and 195.
30. Listening to Prozac, pp. 145-146.
31. Listening to Prozac, p. 177.
32. Listening to Prozac, p. 195.
33. Healy, The Antidepressant Era, op. cit., p.
173.
34. The Confessions of St. Augustine, trans. J. G. Pilkington, Norwalk: Easton Press, 1979, ch.
9, pp. 160-162.
35. Wolterstorff, N., Lament for a Son, Grand Rapids:
Eerdman’s, 1987, pp. 96-97.
36. Huxley, A., Brave New World, Norwalk: Easton Press,
1978.
37. McHugh, P., et al., The Perspectives of Psychiatry, p.
71.
38. Diagnostic and Statistical Manual of Mental Disorders, op.
cit.
==============================
Chapter
6. “Beyond Therapy”: General Reflections
The four preceding chapters have examined how several
prominent and (generally) salutary human pursuits may be aided or altered using
a wide variety of biotechnologies that lend themselves to purposes “beyond
therapy.” In each case, we have discussed the character of the end, considered
the novel means, and explored some possible implications, ethical and social.
In surveying the pertinent technologies, we have taken a somewhat long-range
view, looking at humanly significant technical possibilities that may soon—or
not so soon—be available for general use, yet at the same time trying to
separate fact from science fiction. In offering ethical analysis, we have tried
to identify key issues pertinent to the case under discussion, asking questions
about both ends and means, and looking always for the special significance of
pursuing the old human ends by these new technological means. In this
concluding chapter, we step back from the particular “case studies” to pull
together some common threads and to offer some generalizations and conclusions
to which the overall inquiry has led.
I. The Big
Picture
The first generalization concerns the wide array of
biotechnologies that are, or may conceivably be, useful in pursuing goals
beyond therapy. Although not originally developed for such uses, the available
and possible techniques we have considered—techniques for screening genes and
testing embryos, choosing sex of children, modifying the behavior of children,
augmenting muscle size and strength, enhancing athletic performance, slowing
senescence, blunting painful memories, and brightening mood—do indeed promise
us new powers that can serve age-old human desires. True, in some cases, the
likelihood that the new technologies will be successfully applied to those
purposes seems, at least for the foreseeable future, far-fetched: genetically
engineered “designer babies” are not in the offing. In other cases, as with
psychotropic drugs affecting memory, mood, and behavior, some uses beyond
therapy are already with us. In still other cases, such as research aimed at
retarding senescence, only time will tell what sort of powers may become
available for increasing the maximum human lifespan, and by how much. Yet the
array of biotechnologies potentially useful in these ventures should not be
underestimated, especially when we consider how little we yet know about the
human body and mind and how much our knowledge and technique will surely grow in
the coming years. Once we acquire technical tools and the potential for their
use based on fuller knowledge, we will likely be able to intervene much more
knowingly, competently, and comprehensively.
Second, despite the heterogeneity of the techniques, the
variety of purposes they may serve, and the different issues raised by pursuing
these differing purposes by diverse means, we believe that all of these matters
deserve to be considered together, just as we have done in this report.
Notwithstanding the multiplicity of ends, means, and consequences that we have
considered, this report offers less a list of many things to think about than a
picture of one big thing to think about: the dawning age of
biotechnology and the greatly augmented power it is providing us, not only for
gaining better health but also for improving our natural capacities and
pursuing our own happiness. The ambitious project for the mastery of nature,
the project first envisioned by Francis Bacon and René Descartes in the early
seventeenth century, is finally yielding its promised abilities to relieve man’s
estate—and then some. Though our society will, as a matter of public practice,
be required to deal with each of these techniques and possibilities as they
arrive, piecemeal and independently of one another, we should, as a matter of
public understanding, try to see what they might all add up to, taken together.
The Council’s experience of considering these disparate subjects under this one
big idea—”beyond therapy, for the pursuit of happiness”—and our discovery of
overlapping ethical implications would seem to vindicate the starting
assumption that led us to undertake this project in the first place: biotechnology
beyond therapy deserves to be examined not in fragments, but as a whole.
Yet, third, the “whole” that offers us the most revealing
insights into this subject is not itself technological. For the age of
biotechnology is not so much about technology itself as it is about human
beings empowered by biotechnology. Thus, to understand the human and social
meaning of the new age, we must begin not from our tools and products but from
where human beings begin, namely, with the very human desires that we have here
identified in order to give shape to this report: desires for better children,
superior performance, younger and more beautiful bodies, abler minds, happier
souls. Looking at the big picture through this lens keeps one crucial fact
always in focus: how people exploit the relatively unlimited uses of
biotechnical power will be decisively determined by the perhaps still more
unlimited desires of human beings, especially—and this is a vital point—as
these desires themselves become transformed and inflated by the new
technological powers they are all the while acquiring. Our desires to alter our
consciousness or preserve our youthful strength, perhaps but modest to begin
with, could swell considerably if and when we become more technically able to
satisfy them. And as they grow, what would have been last year’s satisfaction
will only fuel this year’s greater hunger for more.
Fourth, as the ubiquitous human desires are shaped and
colored not only reactively by the tools that might serve them but also
directly by surrounding cultural and social ideas and practices, the “one big
picture” will be colored by the (albeit changeable) ruling opinions, mores, and
institutions of the society in which we live and into which the technologies
are being introduced. For example, the desire for performance-enhancing drugs
will be affected by the social climate regarding competition; the eagerness to
gain an edge for one’s children will be affected by whether many other parents
are doing so; and the willingness to use or forego medication for various sorts
of psychic distress will be affected by the poverty or richness of private
life, and the degree to which strong family or community support is (or is not)
available for coping with that distress directly. Moreover, in a free and
pluralistic society, we may expect a very diverse popular reaction to the
invitation of the new technologies, ranging from exuberant enthusiasm to
outright rejection, and the overall public response cannot be judged in
advance. Yet because the choices made by some can, in their consequences, alter
the shared life lived by all, it behooves all of us to consider the meaning of
these developments, whether we are privately tempted by them or not. It is in
part to contribute to a more thoughtful public appraisal of these possibilities
that we have undertaken this report.
By beginning with the common human desires, we have sought
to place what may be new and strange into a context provided by what is old and
familiar. We recognize the temptation to add biotechnological means to our “tool
kits” for pursuing happiness and self-improvement, and it is not difficult to
appreciate, at least at first glance, the attractiveness of the goods being
contemplated. We want to give our children the best start in life and every
chance to succeed. We want to perform at our best, and better than we did
before. We want to remain youthful and vigorous for as long as we can. We want
to face life optimistically and with proper self-regard. And since we now avail
ourselves of all sorts of means toward these ends, we will certainly not want
to neglect the added advantages that biotechnologies may offer us, today and
tomorrow.
At the same time, however, we have identified, in each of
the previous four chapters, several reasonable sources of concern, ethical and
social. And, in each case, we have called attention to some of the possible
hidden costs of success, achieved by employing these means. The chapter on
better children raised questions about the meaning and limits of parental
control and about the character and rearing of children. The chapter on superior
performance raised questions about the meaning of excellence and the “humanity”
of human activity. The chapter on ageless bodies raised questions about the
significance of the “natural” life cycle and lifespan, and their connection to
the dynamic character of society and the prospects for its invigorating
renewal. And the chapter on happy souls raised questions about the connections
between experienced mood or self-esteem and the deeds or experiences that
ordinarily are their foundation, as well as the connections between remembering
truly and personal identity. Looking again at these subjects, now seen as part
of “one big picture,” we think it useful here to collect and organize the
various issues into a semi-complete account, so that the reader may see in
outline the most important and likely sources of concern.
Before proceeding, we wish to reiterate our intention in
this inquiry, so as to avoid misunderstanding. In offering our synopsis of
concerns, we are not making predictions; we are merely pointing to possible
hazards, hazards that become visible only when one looks at “the big picture.”
More important, we are not condemning either biotechnological power or the
pursuit of happiness, excellence, or self-perfection. Far from it. We eagerly
embrace biotechnologies as aids for preventing or correcting bodily or mental
ills and for restoring health and fitness. We even more eagerly embrace the
pursuits of happiness, excellence, and self-improvement, for ourselves, our
children, and our society. Desires for these goals are the source of much that
is good in human life. Yet, as has long been known, these desires can be
excessive. Worse, they can be badly educated regarding the nature of their
object, sometimes with tragic result: we get what we ask for only to discover
that it is very far from what we really wanted. Finally, they can be pursued in
harmful ways and with improper means, often at the price of deforming the very
goals being sought. To guard against such outcomes, we need to be alert in advance
to the more likely risks and the more serious concerns. We begin with those
that are more obvious and familiar.
II. Familiar
Sources of Concern
The first concerns commonly expressed regarding any uses of
biotechnology beyond therapy reflect, not surprisingly, the dominant values of
modern America: health and safety, fairness and equality, and freedom. The
following thumbnail sketches of the issues should suffice to open the
questions—though of course not to settle them.
A.
Health: Issues of Safety and Bodily Harm
In our health-conscious culture, the first reason people
worry about any new biotechnical intervention, whatever its intended purpose,
is safety. This will surely be true regarding “elective” uses of biotechnology
that aim beyond therapy. Athletes who take steroids to boost their strength may
later suffer premature heart disease. College students who snort Ritalin to
increase their concentration may become addicted. Melancholics taking
mood-brighteners to change their outlook may experience impotence or apathy. To
generalize: no biological agent used for purposes of self-perfection or
self-satisfaction is likely to be entirely safe. This is good medical common
sense: anything powerful enough to enhance system A is likely to be powerful
enough to harm system B (or even system A itself), the body being a highly
complex yet integrated whole in which one intervenes partially only at one’s
peril. And it surely makes sense, ethically speaking, that one should not risk
basic health pursuing a condition of “better than well.”
Yet some of the interventions that might aim beyond
therapy—for example, genetic enhancement of muscle strength, retardation of
aging, or pharmacologic blunting of horrible memories or increasing
self-esteem—may, indirectly, lead also to improvements in general health. More
important, many good things in life are filled with risks, and free people—even
if properly informed about the magnitude of those risks—may choose to run them
if they care enough about what they might gain thereby. If the interventions
are shown to be highly dangerous, many people will (later if not sooner)
avoid them, and the Food and Drug Administration or tort liability will
constrain many a legitimate would-be producer. But if, on the other hand, the
interventions work well and are indeed highly desired, people may freely
accept, in trade-off, even considerable risk of later bodily harm for the sake
of significant current benefits. Besides, the bigger ethical issues in this
area have little to do with safety; the most basic questions concern not the
hazards associated with the techniques but the benefits and harms of using the
perfected powers, assuming that they may be safely used.
B. Unfairness
An obvious objection to the use of enhancement
technologies, especially by participants in competitive activities, is that
they give those who use them an unfair advantage: blood doping or steroids in
athletes, stimulants in students taking the SATs, and so on. This issue,
briefly discussed in Chapter Three, has been well aired by the International
Olympic Committee and the many other athletic organizations who continue to try
to formulate rules that can be enforced, even as the athletes and their
pharmacists continue to devise ways to violate those rules and escape detection.
Yet as we saw, the fairness question can be turned on its head, and some people
see in biotechnical intervention a way to compensate for the “unfairness” of natural
inequalities—say, in size, strength, drive, or native talent. Still, even if
everyone had equal access to genetic improvement of muscle strength or
mind-enhancing drugs, or even if these gifts of technology would be used only
to rectify the inequalities produced by the unequal gifts of nature, an
additional disquiet would still perhaps remain: The disquiet of using such new
powers in the first place or at all, even were they fairly distributed.
Besides, as we have emphasized, not all activities of life are competitive, and
the uses of biotechnologies for purposes beyond therapy are more worrisome on
other grounds.i
C. Equality of Access
A related question concerns inequality of access to the
benefits of biotechnology, a matter of great interest to many Members of this
Council, though little discussed in the previous chapters. The issue of
distributive justice is more important than the issue of unfairness in
competitive activities, especially if there are systemic disparities between
those who will and those who won’t have access to the powers of biotechnical “improvement.”
Should these capabilities arrive, we may face severe aggravations of existing “unfairnesses”
in the “game of life,” especially if people who need certain agents to treat
serious illness cannot get them while other people can enjoy them for less
urgent or even dubious purposes. If, as is now often the case with expensive
medical care, only the wealthy and privileged will be able to gain easy access
to costly enhancing technologies, we might expect to see an ever-widening gap
between “the best and the brightest” and the rest. The emergence of a
biotechnologically improved “aristocracy”—augmenting the already cognitively
stratified structure of American society—is indeed a worrisome possibility, and
there is nothing in our current way of doing business that works against it.
Indeed, unless something new intervenes, it would seem to be a natural outcome
of mixing these elements of American society: our existing inequalities in
wealth and status, the continued use of free markets to develop and obtain the
new technologies, and our libertarian attitudes favoring unrestricted personal
freedom for all choices in private life.
Yet the situation regarding rich and poor is more complex,
especially if one considers actual benefits rather than equality or relative
well-being. The advent of new technologies often brings great benefits to the
less well off, if not at first, then after they come to be mass-produced and
mass-marketed and the prices come down. (Consider, over the past half-century,
the spread in the United States of refrigerators and radios, automobiles and
washing machines, televisions and VCRs, cell phones and personal computers,
and, in the domain of medicine, antibiotics, vaccines, and many expensive
diagnostic and therapeutic procedures.) To be sure, the gap between the richest
and the poorest may increase, but in absolute terms the poor may benefit more,
when compared not to the rich but to where they were before. By many measures,
the average American today enjoys a healthier, longer, safer, and more
commodious life than did many a duke or prince but a few centuries back.
Nevertheless, worries about possible future bio-enhanced
stratification should not be ignored. And they become more poignant in the
present, to the extent that one regards spending money and energy on goals
beyond therapy as a misallocation of limited resources in a world in which the
basic health needs of millions go unaddressed. Yet although the setting of priorities
for research and development is an important matter for public policy, it is
not unique to the domain of “beyond therapy.” It cannot be addressed, much less
solved, in this area alone. Moreover, and yet again, the inequality of access
does not remove our uneasiness over the thing itself. It is, to say the least,
paradoxical, in discussions of the dehumanizing dangers of, say, future eugenic
selection of better children, that people vigorously complain that the poor
will be denied equal access to the danger: “The food is contaminated, but why
are my portions so small?” Huxley’s Brave New World runs on a deplorable
and impermeably rigid class system, but few people would want to live in that
world even if offered the chance to enjoy it as an alpha (the privileged
caste). Even an elite can be dehumanized, can dehumanize itself. The questions
about access and distributive justice are, no doubt, socially important. Yet
the more fundamental ethical questions about taking biotechnology “beyond
therapy” concern not equality of access, but the goodness or badness of the
things being offered and the wisdom of pursuing our purposes by such means.
D. Liberty:
Issues of Freedom and Coercion, Overt and Subtle
A concern for threats to freedom comes to the fore whenever
biotechnical powers are exercised by some people upon other people. We
encountered it in our discussion of “better children” (the choice of a child’s
sex or the drug-mediated alteration of his or her behavior; Chapter Two), as
well as in the coerced use of anabolic steroids by the East German Olympic
swimmers (Chapter Three). This problem will of course be worse in tyrannical
regimes. But there are always dangers of despotism within families, as many
parents already work their wills on their children with insufficient regard to
a child’s independence or long-term needs, jeopardizing even the “freedom to be
a child.” To the extent that even partial control over genotype—say, to take a
relatively innocent example, musician parents selecting a child with genes for
perfect pitch—would add to existing social instruments of parental control and
its risks of despotic rule, this matter will need to be attended to.ii
Leaving aside the special case of children, the risk of
overt coercion does not loom large in a free society. On the contrary, many
enthusiasts for using technology for personal enhancement are libertarian in
outlook; they see here mainly the enlargement of human powers and possibilities
and the multiplication of options for private choice, both of which they see as
steps to greater human freedom. They look forward to growing opportunities for
more people to earn more, learn more, see more, and do more, and to choose—perhaps
several times in one lifetime—interesting new careers or avocations. And they
look with suspicion at critics who they fear might want to limit their private
freedom to develop and use new technologies for personal advancement or,
indeed, for any purpose whatsoever. The coercion they fear comes not from
advances in technology but from the state, acting to deny them their right to
pursue happiness or self-improvement by the means they privately choose.
Yet no one can deny that people living in free societies,
and even their most empowered citizens, already experience more subtle
impingements on freedom and choice, operating, for example, through peer
pressure. What is freely permitted and widely used may, under certain
circumstances, become practically mandatory. If most children are receiving
memory enhancement or stimulant drugs, failure to provide them for your child
might be seen as a form of child neglect. If all the defensive linemen are on
steroids, you risk mayhem if you go against them chemically pure. And, a point
subtler still, some critics complain that, as with cosmetic surgery, Botox, and
breast implants, many of the enhancement technologies of the future will very
likely be used in slavish adherence to certain socially defined and merely
fashionable notions of “excellence” or improvement, very likely shallow and
conformist. If these fears are realized, such exercises of individual freedom,
suitably multiplied, might compromise the freedom to be an individual.iii
This special kind of reduction of freedom—let’s call it the
problem of conformity or homogenization—is of more than individual concern. In
an era of mass culture, itself the by-product of previous advances in
communication, manufacture, and marketing techniques, the exercise of uncoerced
private choices may produce untoward consequences for society as a whole.
Trends in popular culture lead some critics to worry that the self-selected nontherapeutic
uses of the new biotechnical powers, should they become widespread, will be put
in the service of the most common human desires, moving us toward still greater
homogenization of human society—perhaps raising the floor but also lowering the
ceiling of human possibility, and reducing the likelihood of genuine freedom,
individuality, and greatness. (This is an extension of Tocqueville’s concern
about the leveling effects of democracy, now possibly augmented by the
technological power to make those effects ingrained and perhaps irreversible.)
Indeed, such constriction of individual possibility could
be the most important society-wide concern, if we consider the aggregated
effects of the likely individual choices for biotechnical “self-improvement,” each
of which might be defended or at least not objected to on a case-by-case basis
(the problem of what the economists call “negative externalities”). For
example, it might be difficult to object to a personal choice for a
life-extending technology that would extend the user’s life by three healthy
decades or a mood-brightened way of life that would make the individual more
cheerful and untroubled by the world around him. Yet as we have suggested more
than once, the aggregated social effects of such choices, widely made, could
lead to a Tragedy of the Commons, where benefits gained by individuals are
outweighed by the harms that return to them from the social costs of allowing
everyone to share the goodies. And, as Huxley strongly suggests in Brave New
World, when biotechnical powers are readily available to satisfy short-term
desires or to produce easy contentment, the character of human striving changes
profoundly and the desire for human excellence fades. Should this come to pass,
the best thing to be hoped for might be the preservation of pockets of
difference (as on the remote islands in Brave New World) where the
desire for high achievement has not been entirely submerged or eroded.iv
III. Essential
Sources of Concern
Our familiar worries about issues of safety, equality, and
freedom, albeit very important, do not exhaust the sources of reasonable
concern. When richly considered, they invite us to think about the deeper
purposes for the sake of which we want to live safely, justly, and freely. And
they enable us to recognize that even the safe, equally available, non-coerced
and non-faddish uses of biomedical technologies to pursue happiness or
self-improvement raise ethical and social questions, questions more directly
connected with the essence of the activity itself: the use of technological
means to intervene into the human body and mind, not to ameliorate their
diseases but to change and improve their normal workings. Why, if at all, are
we bothered by the voluntary self-administration of agents that would
change our bodies or alter our minds? What is disquieting about our attempts to
improve upon human nature, or even our own particular instance of it?
The subject being relatively novel, it is difficult to put
this worry into words. We are in an area where initial revulsions are hard to
translate into sound moral arguments. Many people are probably repelled by the
idea of drugs that erase memories or that change personalities, or of
interventions that enable seventy-year-olds to bear children or play
professional sports, or, to engage in some wilder imaginings, of mechanical
implants that would enable men to nurse infants or computer-brain hookups that
would enable us to download the Oxford English Dictionary. But can our
disquiet at such prospects withstand rational, anthropological, or ethical
scrutiny? Taken one person at a time, with a properly prepared set of
conditions and qualifications, it will be hard to say what is wrong with any
biotechnical intervention that could improve our performances, give us (more)
ageless bodies, or make it possible for us to have happier souls. Indeed, in
many cases, we ought to be thankful for or pleased with the improvements our
biotechnical ingenuity is making possible.
If there are essential reasons to be concerned about these
activities and where they may lead us, we sense that it may have something to
do with challenges to what is naturally human, what is humanly dignified, or to
attitudes that show proper respect for what is naturally and dignifiedly human.
As it happens, at least four such considerations have already been treated in
one place or another in the previous chapters: appreciation of and respect for “the
naturally given,” threatened by hubris; the dignity of human activity,
threatened by “unnatural” means; the preservation of identity, threatened by
efforts at self-transformation; and full human flourishing, threatened by
spurious or shallow substitutes.
A.
Hubris or Humility: Respect for “the Given”
A common, man-on-the-street reaction to the prospects of
biotechnological engineering beyond therapy is the complaint of “man playing
God.” If properly unpacked, this worry is in fact shared by people holding various
theological beliefs and by people holding none at all. Sometimes the charge
means the sheer prideful presumption of trying to alter what God has ordained
or nature has produced, or what should, for whatever reason, not be fiddled
with. Sometimes the charge means not so much usurping God-like powers, but
doing so in the absence of God-like knowledge: the mere playing at being God,
the hubris of acting with insufficient wisdom.
Over the past few decades, environmentalists, forcefully
making the case for respecting Mother Nature, have urged upon us a “precautionary
principle” regarding all our interventions into the natural world. Go slowly,
they say, you can ruin everything. The point is certainly well taken in the
present context. The human body and mind, highly complex and delicately
balanced as a result of eons of gradual and exacting evolution, are almost
certainly at risk from any ill-considered attempt at “improvement.” There is
not only the matter of unintended consequences, a concern even with interventions
aimed at therapy. There is also the matter of uncertain goals and absent
natural standards, once one proceeds “beyond therapy.” When a physician
intervenes therapeutically to correct some deficiency or deviation from a
patient’s natural wholeness, he acts as a servant to the goal of health and as
an assistant to nature’s own powers of self-healing, themselves wondrous
products of evolutionary selection. But when a bioengineer intervenes for
nontherapeutic ends, he stands not as nature’s servant but as her aspiring
master, guided by nothing but his own will and serving ends of his own
devising. It is far from clear that our delicately integrated natural bodily
powers will take kindly to such impositions, however desirable the sought-for
change may seem to the intervener. And there is the further question of the
unqualified goodness of the goals being sought, a matter to which we shall
return.v
One revealing way to formulate the problem of hubris is
what one of our Council Members has called the temptation to “hyper-agency,” a
Promethean aspiration to remake nature, including human nature, to serve our
purposes and to satisfy our desires. This attitude is to be faulted not only
because it can lead to bad, unintended consequences; more fundamentally, it
also represents a false understanding of, and an improper disposition toward,
the naturally given world. The root of the difficulty seems to be both
cognitive and moral: the failure properly to appreciate and respect the “giftedness”
of the world. Acknowledging the giftedness of life means recognizing that our
talents and powers are not wholly our own doing, nor even fully ours, despite
the efforts we expend to develop and to exercise them. It also means
recognizing that not everything in the world is open to any use we may desire
or devise. Such an appreciation of the giftedness of life would constrain the
Promethean project and conduce to a much-needed humility. Although it is in
part a religious sensibility, its resonance reaches beyond religion.1
Human beings have long manifested both wondering
appreciation for nature’s beauty and grandeur and reverent awe before nature’s
sublime and mysterious power. From the elegance of an orchid to the splendor of
the Grand Canyon, from the magnificence of embryological development to the
miracle of sight or consciousness, the works of nature can still inspire in
most human beings an attitude of respect, even in this age of technology.
Nonetheless, the absence of a respectful attitude is today a problem in
some—though by no means all—quarters of the biotechnical world. It is worrisome
when people act toward, or even talk about, our bodies and minds—or human
nature itself—as if they were mere raw material to be molded according to human
will. It is worrisome when people speak as if they were wise enough to redesign
human beings, improve the human brain, or reshape the human life cycle. In the
face of such hubristic temptations, appreciating that the given world—including
our natural powers to alter it—is not of our own making could induce a welcome
attitude of modesty, restraint, and humility. Such a posture is surely
recommended for anyone inclined to modify human beings or human nature for
purposes beyond therapy.
Yet the respectful attitude toward the “given,” while both
necessary and desirable as a restraint, is not by itself sufficient as a guide.
The “giftedness of nature” also includes smallpox and malaria, cancer and
Alzheimer disease, decline and decay. Moreover, nature is not equally generous
with her gifts, even to man, the most gifted of her creatures. Modesty born of
gratitude for the world’s “givenness” may enable us to recognize that not
everything in the world is open to any use we may desire or devise, but it will
not by itself teach us which things can be tinkered with and
which should be left inviolate. Respect for the “giftedness” of things cannot
tell us which gifts are to be accepted as is, which are to be improved through
use or training, which are to be housebroken through self-command or
medication, and which opposed like the plague.
To guide the proper use of biotechnical power, we need
something in addition to a generalized appreciation for nature’s gifts. We
would need also a particular regard and respect for the special gift that is
our own given nature. For only if there is a human “givenness,” or a
given humanness, that is also good and worth respecting, either as we find it
or as it could be perfected without ceasing to be itself, will the “given”
serve as a positive guide for choosing what to alter and what to leave
alone. Only if there is something precious in our given human nature—beyond the
fact of its giftedness—can what is given guide us in resisting efforts that
would degrade it. When it comes to human biotechnical engineering beyond
therapy, only if there is something inherently good or dignified about, say,
natural procreation, the human life cycle (with its rhythm of rise and fall),
and human erotic longing and striving; only if there is something inherently
good or dignified about the ways in which we engage the world as spectators and
appreciators, as teachers and learners, leaders and followers, agents and
makers, lovers and friends, parents and children, citizens and worshippers, and
as seekers of our own special excellence and flourishing in whatever arena to
which we are called—only then can we begin to see why those aspects of our
nature need to be defended against our deliberate redesign.
We must move, therefore, from the danger of hubris in the
powerful designer to the danger of degradation in the designed, considering how
any proposed improvements might impinge upon the nature of the one being
improved. With the question of human nature and human dignity in mind, we move
to questions of means and ends.
B.
“Unnatural” Means: The Dignity of Human Activity
Until only yesterday, teaching and learning or practice and
training exhausted the alternatives for acquiring human excellence, perfecting
our natural gifts through our own efforts. But perhaps no longer: biotechnology
may be able to do nature one better, even to the point of requiring less teaching,
training, or practice to permit an improved nature to shine forth. As we noted
earlier, the insertion of the growth-factor gene into the muscles of rats and
mice bulks them up and keeps them strong and sound without the need for nearly
as much exertion. Drugs to improve alertness (today) or memory and amiability
(tomorrow) could greatly relieve the need for exertion to acquire these powers,
leaving time and effort for better things. What, if anything, is disquieting
about such means of gaining improvement?
The problem cannot be that they are “artificial,” in the
sense of having man-made origins. Beginning with the needle and the fig leaf,
man has from the start been the animal that uses art to improve his lot by
altering or adding to what nature alone provides.vi
Ordinary medicine makes extensive use of similar artificial means, from drugs
to surgery to mechanical implants, in order to treat disease. If the use of artificial
means is absolutely welcome in the activity of healing, it cannot be their
unnaturalness alone that disquiets us when they are used to make people “better
than well.”
Still, in those areas of human life in which excellence has
until now been achieved only by discipline and effort, the attainment of
similar results by means of drugs, genetic engineering, or implanted devices
looks to many people (including some Members of this Council) to be “cheating”
or “cheap.” Many people believe that each person should work hard for his
achievements. Even if we prefer the grace of the natural athlete or the
quickness of the natural mathematician—people whose performances deceptively
appear to be effortless—we admire also those who overcome obstacles and struggle
to try to achieve the excellence of the former. This matter of character—the
merit of disciplined and dedicated striving—is surely pertinent. For character
is not only the source of our deeds, but also their product. As we have already
noted, healthy people whose disruptive behavior is “remedied” by pacifying
drugs rather than by their own efforts are not learning self-control;vii
if anything, they may be learning to think it unnecessary. People who take
pills to block out from memory the painful or hateful aspects of a new
experience will not learn how to deal with suffering or sorrow. A drug that
induces fearlessness does not produce courage.
Yet things are not so simple. Some biotechnical
interventions may assist in the pursuit of excellence without in the least
cheapening its attainment. And many of life’s excellences have nothing to do
with competition or overcoming adversity. Drugs to decrease drowsiness, increase
alertness, sharpen memory, or reduce distraction may actually help people
interested in their natural pursuits of learning or painting or performing
their civic duty. Drugs to steady the hand of a neurosurgeon or to prevent
sweaty palms in a concert pianist cannot be regarded as “cheating,” for they
are in no sense the source of the excellent activity or achievement. And, for
people dealt a meager hand in the dispensing of nature’s gifts, it should not
be called cheating or cheap if biotechnology could assist them in becoming
better equipped—whether in body or in mind.
Nevertheless, as we suggested at some length in Chapter
Three, there remains a sense that the “naturalness” of means matters. It lies
not in the fact that the assisting drugs and devices are artifacts, but in the
danger of violating or deforming the nature of human agency and the dignity of
the naturally human way of activity. In most of our ordinary efforts at
self-improvement, whether by practice, training, or study, we sense the relation
between our doings and the resulting improvement, between the means used and
the end sought. There is an experiential and intelligible connection between
means and ends; we can see how confronting fearful things might eventually
enable us to cope with our fears. We can see how curbing our appetites produces
self-command. Human education ordinarily proceeds by speech or symbolic deeds,
whose meanings are at least in principle directly accessible to those upon whom
they work.
In contrast, biotechnical interventions act directly on the
human body and mind to bring about their effects on a passive subject, who
plays little or no role at all. He can at best feel their effects without
understanding their meaning in human terms. Thus, a drug that brightened
our mood would alter us without our understanding how and why it did so—whereas
a mood brightened as a fitting response to the arrival of a loved one or to an
achievement in one’s work is perfectly, because humanly, intelligible. And not
only would this be true about our states of mind. All of our encounters with
the world, both natural and interpersonal, would be mediated, filtered, and
altered. Human experience under biological intervention becomes increasingly
mediated by unintelligible forces and vehicles, separated from the human
significance of the activities so altered. The relations between the knowing
subject and his activities, and between his activities and their fulfillments
and pleasures, are disrupted.
The importance of human effort in human achievement is here
properly acknowledged: the point is less the exertions of good character
against hardship, but the manifestation of an alert and self-experiencing agent
making his deeds flow intentionally from his willing, knowing, and embodied
soul. If human flourishing means not just the accumulation of external
achievements and a full curriculum vitae but a lifelong being-at-work
exercising one’s human powers well and without great impediment,
our genuine happiness requires that there be little gap, if any, between the
dancer and the dance.viii
C.
Identity and Individuality
With biotechnical interventions that skip the realm of
intelligible meaning, we cannot really own the transformations nor can we
experience them as genuinely ours. And we will be at a loss to attest whether
the resulting conditions and activities of our bodies and our minds are, in the
fullest sense, our own as human. But our interest in identity is also more
personal. For we do not live in a generic human way; we desire, act, flourish,
and decline as ourselves, as individuals. To be human is to be someone,
not anyone—with a given nature (male or female), given natural abilities
(superior wit or musical talent), and—most important—a real history of
attachments, memories, and experiences, acquired largely by living with others.
In myriad ways, new biotechnical powers promise (or
threaten) to transform what it means to be an individual: giving increased
control over our identity to others, as in the case of genetic screening or sex
selection of offspring by parents; inducing psychic states divorced from real
life and lived experience; blunting or numbing the memories we wish to escape;
and achieving the results we could never achieve unaided, by acting as
ourselves alone.
To be sure, in many cases, biomedical technology can
restore or preserve a real identity that is slipping away: keeping our memory
intact by holding off the scourge of Alzheimer disease; restoring our capacity
to love and work by holding at bay the demons of self-destroying depression. In
other cases, the effect of biotechnology on identity is much more ambiguous. By
taking psychotropic drugs to reduce anxiety or overcome melancholy, we may
become the person we always wished to be—more cheerful, ambitious, relaxed,
content. But we also become a different person in the eyes of others, and in
many cases we become dependent on the continued use of psychotropic drugs to
remain the new person we now are.
As the power to transform our native powers increases, both
in magnitude and refinement, so does the possibility for “self-alienation”—for
losing, confounding, or abandoning our identity. I may get better, stronger,
and happier—but I know not how. I am no longer the agent of
self-transformation, but a passive patient of transforming powers. Indeed, to
the extent that an achievement is the result of some extraneous intervention,
it is detachable from the agent whose achievement it purports to be. “Personal
achievements” impersonally achieved are not truly the achievements of persons.
That I can use a calculator to do my arithmetic does not make me a
knower of arithmetic; if computer chips in my brain were to “download” a
textbook of physics, would that make me a knower of physics? Admittedly,
the relation between biological boosters and personal identity is much less
clear: if I make myself more alert through Ritalin, or if drugs can make up for
lack of sleep, I may be able to learn more using my unimpeded native powers
while it is still unquestionably I who am doing the learning. And yet,
to find out that an athlete took steroids before the race or that a test-taker
(without medical disability) took Ritalin before the test is to lessen our regard
for the achievement of the doer. It is to see not just an acting self, but a
dependent self, one who is less himself for becoming so dependent.
In the deepest sense, to have an identity is to have
limits: my body, not someone else’s—even when the pains of aging might tempt me
to become young again; my memories, not someone else’s—even when the traumas of
the past might tempt me to have someone else’s memories; my achievements and
potential, not someone else’s—even when the desire for excellence might tempt
me to “trade myself in” for a “better model.” We seek to be happy—to achieve,
perform, take pleasure in our experiences, and catch the admiring eye of a
beloved. But we do not, at least self-consciously, seek such happiness at the
cost of losing our real identity.
D.
Partial Ends, Full Flourishing
Beyond the perils of achieving our desired goals in a “less-than-human
way” or in ways “not fully our own,” we must consider the meaning of the ends
themselves: better children, superior performance, ageless bodies, and happy
souls. Would their attainment in fact improve or perfect our lives as human
beings? Are they—always or ever—reasonable and attainable goals?
Everything depends, as we have pointed out in each case, on
how these goals are understood, on their specific and concrete content. Yet,
that said, the first two human ends—better children and superior performance—do
seem reasonable and attainable, sometimes if not always, to some degree if not
totally. When asked what they wish for their children, most parents say: “We
want them to be happy,” or “We want them to live good lives”—in other words, to
be better and to do better. The desire is a fitting one for any loving parent.
The danger lies in misconceiving what “better children” really means, and thus
coming to pursue this worthy goal in a misguided way, or with a false idea of
what makes for a good or happy child.
Likewise, the goal of superior performance—the desire to be
better or do better in all that we do—is good and noble, a fitting human
aspiration. We admire excellence whenever we encounter it, and we properly seek
to excel in those areas of life, large and small, where we ourselves are
engaged and at-work. But the danger here is that we will become better in some
area of life by diminishing ourselves in others, or that we will achieve
superior results only by compromising our humanity, or by corrupting those
activities that are not supposed to be “performances” measured in terms of
external standards of “better and worse.”
In many cases, biotechnologies can surely help us cultivate
what is best in ourselves and in our children, providing new tools for
realizing good ends, wisely pursued. But it is also possible that the new
technological means may deform the ends themselves. In pursuit of better
children, biotechnical powers risk making us “tyrants”; in pursuit of superior
performance, they risk making us “artifacts.” In both cases, the problem is not
the ends themselves but our misguided idea of their attainment or our false way
of seeking to attain them. And in both cases, there is the ubiquitous problem
that “good” or “superior” will be reconceived to fit the sorts of goals that
the technological interventions can help us attain. We may come to believe that
genetic predisposition or brain chemistry holds the key to helping our children
develop and improve, or that stimulant drugs or bulkier muscles hold the key to
excellent human activity. If we are equipped with hammers, we will see only
those things that can be improved by pounding.
The goals of ageless bodies and happy souls—and especially
the ways biotechnology might shape our pursuit of these ends—are perhaps more
complicated.2
The case for ageless bodies seems at first glance to look pretty good. The
prevention of decay, decline, and disability, the avoidance of blindness,
deafness, and debility, the elimination of feebleness, frailty, and fatigue,
all seem to be conducive to living fully as a human being at the top of one’s
powers—of having, as they say, a “good quality of life” from beginning to end.
We have come to expect organ transplantation for our worn-out parts. We will
surely welcome stem-cell-based therapies for regenerative medicine, reversing
by replacement the damaged tissues of Parkinson disease, spinal cord injury,
and many other degenerative disorders. It is hard to see any objection to
obtaining a genetic enhancement of our muscles in our youth that would not only
prevent the muscular feebleness of old age but would empower us to do any
physical task with greater strength and facility throughout our lives. And,
should aging research deliver on its promise of adding not only extra life to
years but also extra years to life, who would refuse it?
But as we suggested in Chapter Four, there may in fact be
many human goods that are inseparable from our aging bodies, from our living in
time, and especially from the natural human life cycle by which each generation
gives way to the one that follows it. Because this argument is so
counterintuitive, we need to begin not with the individual choice for an
ageless body, but with what the individual’s life might look like in a world in
which everyone made the same choice. We need to make the choice universal, and
see the meaning of that choice in the mirror of its becoming the norm.
What if everybody lived life to the hilt, even as they
approached an ever-receding age of death in a body that looked and
functioned—let’s not be too greedy—like that of a thirty-year-old? Would it be
good if each and all of us lived like light bulbs, burning as brightly from
beginning to end, then popping off without warning, leaving those around us
suddenly in the dark? Or is it perhaps better that there be a shape to life,
everything in its due season, the shape also written, as it were, into the
wrinkles of our bodies that live it—provided, of course, that we do not suffer
years of painful or degraded old age and that we do not lose our wits? What
would the relations between the generations be like if there never came a point
at which a son surpassed his father in strength or vigor? What incentive would
there be for the old to make way for the young, if the old slowed down little
and had no reason to think of retiring—if Michael could play basketball until
he were not forty but eighty? Might not even a moderate prolongation of
lifespan with vigor lead to a prolongation in the young of functional
immaturity—of the sort that has arguably already accompanied the great increase
in average life expectancy experienced in the past century?ix
Going against both common intuition and native human
desire, some commentators have argued that living with full awareness and
acceptance of our finitude may be the condition of many of the best things in
human life: engagement, seriousness, a taste for beauty, the possibility of
virtue, the ties born of procreation, the quest for meaning.3
This might be true not just for immortality—an unlikely achievement, likely to
produce only false expectations—but even for more modest prolongations of the
maximum lifespan, especially in good health, that would permit us to live as if
there were always tomorrow. The pursuit of perfect bodies and further
life-extension might deflect us from realizing more fully the aspirations to
which our lives naturally point, from living well rather than merely staying
alive. A concern with one’s own improving agelessness might finally be
incompatible with accepting the need for procreation and human renewal. And far
from bringing contentment, it might make us increasingly anxious over our
health or dominated by the fear of death. Assume, merely for the sake of the
argument, that even a few of these social consequences would follow from a
world of much greater longevity and vigor: What would we then say about the
simple goodness of seeking an ageless body?
What about the pursuit of happy souls, and especially of
the sort that we might better attain with pharmacological assistance? Painful
and shameful memories are disturbing; guilty consciences trouble sleep; low
self-esteem, melancholy, and world-weariness besmirch the waking hours. Why not
memory-blockers for the former, mood-brighteners for the latter, and a good
euphoriant—without risks of hangovers or cirrhosis—when celebratory occasions
fail to be jolly? For let us be clear: If it is imbalances of neurotransmitters
that are largely responsible for our state of soul, would it not be sheer
priggishness to refuse the help of pharmacology for our happiness, when we
accept it guiltlessly to correct for an absence of insulin or thyroid hormone?
And yet, as we suggested in Chapter Five, there seems to be
something misguided about the pursuit of utter and unbroken psychic tranquility
or the attempt to eliminate all shame, guilt, and painful memories. Traumatic
memories, shame, and guilt, are, it is true, psychic pains. In extreme doses,
they can be crippling. Yet, short of the extreme, they can also be helpful and
fitting. They are appropriate responses to horror, disgraceful conduct,
injustice, and sin, and, as such, help teach us to avoid them or fight against
them in the future. Witnessing a murder should be remembered as horrible; doing
a beastly deed should trouble one’s soul. Righteous indignation at injustice
depends on being able to feel injustice’s sting. And to deprive oneself of one’s
memory—including and especially its truthfulness of feeling—is to deprive
oneself of one’s own life and identity.
These feeling states of soul, though perhaps accompaniments
of human flourishing, are not its essence. Ersatz pleasure or feelings of self-esteem
are not the real McCoy. They are at most shadows divorced from the underlying
human activities that are the essence of flourishing. Most people want both to
feel good and to feel good about themselves, but only as a result of being good
and doing good.
At the same time, there appears to be a connection between
the possibility of feeling deep unhappiness and the prospects for achieving
genuine happiness. If one cannot grieve, one has not truly loved. To be capable
of aspiration, one must know and feel lack. As Wallace Stevens put it: Not to
have is the beginning of desire. In short, if human fulfillment depends on our
being creatures of need and finitude and therewith of longings and attachment,
there may be a double-barreled error in the pursuit of ageless bodies and
factitiously happy souls: far from bringing us what we really need, pursuing
these partial goods could deprive us of the urge and energy to seek a richer
and more genuine flourishing.
Looking into the future at goals pursuable with the aid of
new biotechnologies enables us to turn a reflective glance at our own version
of the human condition and the prospects now available to us (in principle) for
a flourishing human life. For us today, assuming that we are blessed with good
health and a sound mind, a flourishing human life is not a life lived with an
ageless body or an untroubled soul, but rather a life lived in rhythmed time,
mindful of time’s limits, appreciative of each season and filled first of all
with those intimate human relations that are ours only because we are born,
age, replace ourselves, decline, and die—and know it. It is a life of
aspiration, made possible by and born of experienced lack, of the disproportion
between the transcendent longings of the soul and the limited capacities of our
bodies and minds. It is a life that stretches towards some fulfillment to which
our natural human soul has been oriented, and, unless we extirpate the source,
will always be oriented. It is a life not of better genes and enhancing chemicals
but of love and friendship, song and dance, speech and deed, working and
learning, revering and worshipping.
If this is true, then the pursuit of an ageless body may
prove finally to be a distraction and a deformation. And the pursuit of an
untroubled and self-satisfied soul may prove to be deadly to desire, if
finitude recognized spurs aspiration and fine aspiration acted upon is
itself the core of happiness. Not the agelessness of the body, nor the
contentment of the soul, nor even the list of external achievements and
accomplishments of life, but the engaged and energetic being-at-work of what
nature uniquely gave to us is what we need to treasure and defend. All other “perfections”
may turn out to be at best but passing illusions, at worst a Faustian bargain
that could cost us our full and flourishing humanity.
Summing up these “essential sources of concern,” we might
succinctly formulate them as follows:
In wanting to become more than we are, and in sometimes
acting as if we were already superhuman or divine, we risk despising what we
are and neglecting what we have.
In wanting to improve our bodies and our minds using new
tools to enhance their performance, we risk making our bodies and minds little
different from our tools, in the process also compromising the distinctly human
character of our agency and activity.
In seeking by these means to be better than we are or to
like ourselves better than we do, we risk “turning into someone else,”
confounding the identity we have acquired through natural gift cultivated by
genuinely lived experiences, alone and with others.
In seeking brighter outlooks, reliable contentment, and
dependable feelings of self-esteem in ways that by-pass their usual natural
sources, we risk flattening our souls, lowering our aspirations, and weakening
our loves and attachments.
By lowering our sights and accepting the sorts of
satisfactions that biotechnology may readily produce for us, we risk turning a
blind eye to the objects of our natural loves and longings, the pursuit of
which might be the truer road to a more genuine happiness.
To avoid such outcomes, our native human desires need to be
educated against both excess and error. We need, as individuals and as a
society, to find these boundaries and to learn how to preserve and defend them.
To do so in an age of biotechnology, we need to ponder and answer questions
like the following:
When does parental desire for better children constrict
their freedom or undermine their long-term chances for self-command and genuine
excellence?
When does the quest for self-improvement make the “self”
smaller or meaner?
When does a preoccupation with youthful bodies or longer
life jeopardize the prospects for living well?
When does the quest for contentment or self-esteem lead us away
from the activities and attachments that prove to be essential to these goals
when they are properly understood?
Answers to these questions are not easily given in the
abstract or in advance. Boundaries are hard to define in the absence of better
knowledge of the actual hazards. Such knowledge will be obtainable only in time
and only as a result of lived experience. But centrally important in shaping
the possible future outcomes will be the cultural attitudes and social
practices that shape desires, govern expectations, and influence the choices
people make, now and in the future. This means reflecting more specifically on
how biotechnology beyond therapy might affect and be affected by American
society.
IV.
Biotechnology and American Society
In free societies such as our own, choices about using
biotechnologies are not made by central planners looking to realize some dream
of a more perfect future society. They are made largely by private individuals
looking to realize their personal dream of a better life, for themselves and
for their children. The choices that they make will, of course, be constrained
by boundaries set by law and by the limits of their own resources. More subtly,
they will be influenced by the social norms, cultural ideals, and institutional
practices of their communities—as these norms, ideals, and practices are
themselves reciprocally shaped by the aggregated results of countless private
choices. No account of our subject would be complete without a brief look at
these larger social implications.
Looking over the horizon, what sort of society might we be
getting in the coming age of biotechnology? What sort of society are we, in
fact, bringing into being, knowingly or unknowingly, by our private choices?
And how might our existing American norms, ideals, and practices frame and
color the “big picture” whose outlines are only now becoming visible?
On the optimistic view, the emerging picture is one of
unmitigated progress and improvement, yielding a society in which more and more
people are able to realize the American dream of liberty, prosperity, and
justice for all. Projecting that the present century will continue the
remarkable achievements of the one just ended, it is easy to imagine a society
whose citizens are healthier, longer-lived, livelier, freer, more competent,
better educated, more productive, better accomplished, and happier than they
have ever been in any society now known, including our own. Many more human
beings—now biologically better equipped, aided by performance-enhancers, and
more liberated from the constraints of nature and fortune—might someday live on
a much higher human plane than has hitherto been possible save for very few
people. This rosy picture of the future, encouraged by our past successes, cannot
be lightly gainsaid.
Yet, as we have suggested throughout this report, there are
reasons to expect more mixed or even unattractive outcomes. For example, there
are risks—small in today’s United States—of a sex-unbalanced society, the
result of unrestrained free choice in selecting the sex of children; or of a
change-resisting gerontocracy, with the “elders” still young in body but old
and tired in outlook. And there are still uglier possibilities: an increasingly
stratified and inegalitarian society, now with purchased biological
enhancements, with enlarged gaps between the over-privileged few and the
under-privileged many; a society of narcissists focused on personal
satisfaction and self-regard, with little concern for the next generation or
the common good; a society of social conformists but with shallow attachments,
given over to cosmetic fashions and trivial pursuits; or a society of fiercely
competitive individuals, caught up in an ever-spiraling struggle to get ahead,
using the latest biotechnical assistance both to perform better and to deal
with the added psychic stress.
Lacking prophetic powers, we will not hazard any guesses as
to which of these prospects is more likely to be our future. Up until now, such
visionary work has been best left to the imaginative gifts of science fiction
writers, who, more than everyone else, have thought seriously aboutwhere
biotechnology may be taking us, for better and for worse. From now on, however,
we will do well to pay attention to this matter, devising the sorts of social
indicators and empirical research that could teach us which way the social and
cultural winds are blowing.
But if we can only dimly perceive our possible or likely
futures, we can clearly recognize some features of contemporary American life
that will, almost certainly, exercise great influence over the future that is
likely to emerge. Among them we would identify the importance of commerce, the
practice of medicine, and the ruling ideals and ethos of the American polity.
They are already playing major roles in determining which of the many possible
social futures our grandchildren and great-grandchildren will inherit.
A. Commerce, Regulation, and the Manufacture of Desire
Whether one likes it or not, progress in biology and
biotechnology is now intimately bound up with industry and commerce. Although
the federal government is still the major sponsor of biomedical research, more
and more scientists work in partnership with industry. And the emergence of a
vigorous biotech industry, growing rapidly even before it has delivered very
much of its great promise, is a sign of things to come. Whatever one finally
thinks about the relative virtues and vices of contemporary capitalism, it is a
fact that progress in science and technology owes much to free enterprise. The
possibility of gain adds the fuel of interest to the fire of genius, and even
as the profits accrue only to some, the benefits are, at least in principle,
available to all. And the competition to succeed provides enormous incentives
to innovation, growth, and progress. We have every reason to expect exponential
increases in biotechnologies and, therefore, in their potential uses in all
aspects of human life.
Two aspects of the marriage between biotechnology and
free-market commerce pose challenges to our ability to keep control of how
those powers will be used. First, scientists and entrepreneurs, for perfectly
understandable reasons, want no interference with research or development.
Freedom to experiment is essential to discovery; freedom to invent and to
market is essential to technological advance. Distrustful of governmental
regulation and leery of public scrutiny of their activities, biologists and
technologists are especially inclined to resist legal limitations that might be
imposed on their activities based on ethical considerations. Like those who
would prefer to “go slow,” they vigorously make their interests felt in the
deliberations of government. Yet in the long run, as members of American
society, they have as much to gain or lose as anyone else from the kind of
society that their own efforts are helping to create. What sort of society it
will be will depend in part on whether industry and the broader public will
collaborate in finding ways to monitor and regulate the uses of biotechnology
beyond therapy.
Entrepreneurs not only resist governmental limitation of
their work or restrictions on the uses to which their products may be put. They
also promote public demand. The success of enterprise often turns on
anticipating and stimulating consumer demand, sometimes even on creating it
where none exists. Suitably stimulated, the demand of consumers for easier
means to better-behaved children, more youthful or beautiful or potent bodies,
keener or more focused minds, and steadier or more cheerful moods is
potentially enormous. If the existing cosmetic industry may be taken as a
model, the sky may be the limit for a truly effective “cosmetic pharmacology”
that would deliver stronger muscles, better memories, brighter moods, and peace
of mind. The direct-to-consumer advertising of pharmaceutical and other
companies—for mood-brighteners, fatigue lesseners, youth preservatives, and
behavior modifiers—is a harbinger of things to come. Today it is Ritalin,
Botox, Rogaine, Viagra, and Prozac; could tomorrow be “Memorase,” “Popeye’s
Potion,” “Eroticor,” “Self-love,” or “Soma”? Desires can be manufactured almost
as effectively as pills, especially if the pills work more or less as promised
to satisfy the newly stimulated desires. By providing quick solutions for
short-term problems or prompt fulfillment of easily satisfied desires, the
character of human longing itself could be altered, with large aspirations for
long-term flourishing giving way before the immediate gratification of smaller
desires. What to do about this is far from clear; but its importance should not
be underestimated.
B.
Medicine, Medicalization, and a Stance “Beyond Therapy”
Wherever they may be invented and manufactured, most new
biotechnologies, including those serving goals beyond therapy, will probably
enter ordinary use through the offices of the medical profession. Should this
occur, the pursuit of happiness and self-perfection would become part of the
doctor’s business, joining many other aspects of human life that formerly had
little to do with doctors and hospitals: childbirth, infertility, sexual mores
and practices, aspects of criminal behavior, alcoholism, abnormal behavior,
anxiety, stress, dementia, old age, death, grief, and mourning—all these have over
the past century been at least partially medicalized, and often with good
reasons and welcome results.x
The causes of medicalization are many, among them, the power of modern
biological explanation and technique; the growth in medical knowledge and
competence; the expanding domain of psychiatry, the “doctoring of the psyche”;
increased success using medical interventions; and rising patient expectations
of cure, relief, and salvation coming from health care professionals. It is
also driven by deep cultural and intellectual currents, for example, to see
more and more things in life not as natural givens to be coped with but as
objects rightly subject to our mastery and control; to have compassion for
victims, even when the victims are victimized by their own foolish conduct; to
see the human person not in spiritual or moral terms, but as a highly complex
and successful product of blind evolutionary forces (which still perturb him
through no fault of his own); and—very important—the acceptance of “health” as
the one readily recognized and utterly uncontroversial human good (in contrast,
say, with virtue, morality, or wisdom). With the decline in the cultural
authority of religious institutions, and with the shrinking of other communal
systems of help and support for people in difficulty, physicians often find
themselves simply “neighbor to the problem.” Rightly extending a helping hand,
they often conceive and treat the problems they encounter in a purely medical
fashion.
As new biotechnologies appear, with novel uses beyond
therapy, the tendency toward medicalization will almost certainly be
strengthened, both as a matter of practice and as a matter of thought.
Physicians are the gatekeepers of biomedical technologies. They are judges of
proper use. They are aware of dangerous side effects. They prescribe and
dispense as they see fit. The medical profession is clothed in venerable
ethical dress; in the United States there are also professional standards of
good practice that offer guidance and principles of reimbursement that set
limits on free professional and patient choices. Nevertheless, the practice of
medicine is highly decentralized, and each physician has enormous discretion in
dealing with patients, able to adapt general practices to the special needs and
circumstances of each individual. All this is comforting and reassuring, more
so than if the new biotechnical powers were wielded by an upstart group of
technicians lacking these professional assets and virtues.
But there are difficulties when medical practice moves
beyond therapy. Where the goal is restoring health, the doctor’s discretion is
guided by an agreed-upon and recognizable target. But a physician prescribing
for goals beyond therapy is in uncharted waters. Although fully armed with the
means, he has no special expertise regarding the end—neither what it is nor
whether it is desirable. To the extent that the patient is transformed from a
sick person needing healing into a consumer of technical services, medicine
will be transformed from a profession into a trade and the doctor-patient
relationship into a species of contract, ungoverned by any deep ethical norms.
Should this occur, the medical profession and the health care system will be
called upon to practice retail sanity regarding the technologies and wholesale
madness regarding the ends, the costs, and the possible consequences of their
use. The health-care system in the United States already constitutes roughly
one-sixth of the gross national product. What might it become in the coming age
beyond therapy?
There is yet a second and perhaps more fundamental danger
in the growth of medicalization, a danger of thinking and outlook whose
consequences could well be profound. The therapeutic intention at the heart of
medicine—the goal of making whole that which is broken or disabled—runs the
risk of looking increasingly upon the entire human condition in this way and,
as a result, of regarding biotechnological measures as the royal road to
improving our lot in life. Two opposing dangers need to be avoided. On the one
hand, there is the risk of viewing everything in human life—not only human
frailties, disappointments, and death itself, but also human relationships,
pride and shame, love and sorrow, and all self-discontent—under the lens of
disease and disability. Such a tendency would encourage everywhere the idea of
human life as “victimhood” in need of rescue; it would discourage everywhere
the idea that human beings are responsible agents and, at their best, noble
creatures aspiring to and capable of genuine excellence and flourishing. On the
other hand, there is the risk of attacking human limitation altogether, seeking
to produce a more-than-human being, one not only without illnesses, but also
without foibles, fatigue, failures, or foolishness.xi
Seen against these problematic temptations, the remedy for
the dangers lurking in the drift toward greater medicalization and “beyond
therapy” is, paradoxically, to be found in rethinking the very idea of “beyond
therapy.” It is to be found in adopting a standpoint toward human life that is,
in another sense of the term, radically beyond therapy. It does not
start with medicine to discover the terrain that lies beyond the goals of
medicine. It looks beyond the therapeutic view of life altogether. It rejects
and goes beyond the “therapy versus enhancement” distinction for a reason
deeper than those we gave at the outset of this report (see Chapter One): for
medicine, sickness, and healing are not the natural or best lens through which
to look upon the whole of human life. Health, though a primary human good, is
not the only—or even the supreme—human good.
Going “beyond therapy” in this sense means returning to an
account of the human being seen not in material or mechanistic or medical terms
but in psychic and moral and spiritual ones. It is to see the human being as a
creature “in-between,” neither god nor beast, neither dumb body nor disembodied
soul, but as a puzzling, upward-pointing unity of psyche and soma whose precise
limitations are the source of its—our—loftiest aspirations, whose weaknesses
are the source of its—our—keenest attachments, and whose natural gifts may be,
if we do not squander or destroy them, exactly what we need to flourish and
perfect ourselves—as human beings. Readers, we hope, will recognize that
this entire report has been written from this more-than-therapeutic perspective
and with this richly humanistic intent.
C.
Biotechnology and American Ideals
The significance of these two prominent features of
American life—the power of free markets and the prestige of medicine—points us
also toward a greater understanding of the implications of our new biotechnical
powers for our American ideals. In a certain sense, as a people committed to
life, liberty, and the pursuit of happiness, we may tend to be especially drawn
to the promise of biotechnology. Some of the techniques we have discussed offer
the prospect of longer and livelier life, of expanded liberty made possible by
improved abilities and powers, and of a more successful and fulfilling pursuit
of happiness. Medicine thrives in a culture that values life; science and
enterprise thrive in a society that values freedom; technology flourishes in a
nation eager to make life more prosperous and comfortable.
And yet, these very ideals also offer reasons to moderate
the desires that drive us toward greater biotechnological prowess, and to look
upon new possibilities through the lens of a rich yet temperate understanding
of the human condition. Even as they encourage progress, the American
principles may serve to moderate a dangerous utopianism. Our devotion to life
is understood in light of the human dedication to the good life, and so
calls for reflection on our most basic priorities, and on just what it is that
gives life its significance. Our aspiration to liberty is grounded in some
sense that we men and women are the beings deserving of liberty, and capable of
using it well. It reminds us, also, that our actions always run the risk of
curtailing the freedom of others, including especially that of future
generations—to whom we owe the same liberty passed down to us. And our nation’s
declared commitment to the pursuit of happiness—understood in light of our
devotion to life, and our dedication to meaningful liberty—invites us to
consider the nature (and also the limits) of happiness, and to wonder what sort
of happiness a people so devoted and dedicated might rightly pursue.
But these American ideals, and the character of the nation
they have helped to shape, moderate not only our hopes but also our fears. The
reservations we have raised in this report are the worries of a free and decent
people—concerned for its character and its goodness and its soul. Had we looked
only at the perils of the technologies that seem to lie in our future, and had
we sought to imagine the worst, it would not have been difficult to raise up
specters of terrifying and inhuman violations, or of an unprecedented despotism
of man over man, with powerful new technologies serving as the whips of new
slave-masters. The recent history of the human race offers no dearth of sources
for such nightmarish visions. But that is not what we perceive when we peer
over the horizon, because our society, dedicated as it is to life and liberty
and happiness, is always alert to repel such excesses.
Rather, the concerns we have raised here emerge from a
sense that tremendous new powers to serve certain familiar and often
well-intentioned desires may blind us to the larger meaning of our ideals, and
may narrow our sense of what it is to live, to be free, and to seek after
happiness. If, by informing and moderating our desires and by grasping the
limits of our new powers, we can keep in mind the meaning of our founding
ideals, then we just might find the means to savor some fruits of the age of
biotechnology, without succumbing to its most dangerous temptations.
To do so, we must first understand just what is at stake,
and we must begin to imagine what the age of biotechnology might bring, and
what human life in that age could look like. In these pages, we have sought to
begin that vital project, in the hope that these first steps might spark and
inform a public debate, so that however the nation proceeds, it will do so with
its eyes wide open.
_______________
Footnotes
i. For example: It mattered to the young woman we cited in Chapter
Five that the
young man said he loved her only because he was high on Ecstasy. It matters to
all of us that the people we have dealings with are not psychotropically out of
their right minds. In neither case is the issue one of unfair advantage.
ii. The danger of despotism of one generation over the next is, in
fact, one of the arguments sometimes voiced against human cloning. See our
report, Human Cloning and Human Dignity: An Ethical Inquiry, Washington,
D.C.: Government Printing Office, 2002.
iii. Freedom does not automatically increase with a growing range
of options. On the contrary, if the options differ but little from one another
(Nike rather than Adidas, Budweiser rather than Coors), and if the choosing
agent expends growing energies on choices that contribute but little to his or
her genuine well-being, enjoying one’s greater number of options might
represent a curtailment of a deeper and more genuine freedom.
iv.Which of the imaginable social consequences will in fact occur
is, of course, an empirical question, though it is worthwhile to think about
the alternatives in advance. Indeed, anticipatory reflection might play a role
in helping to forestall some of the worst possible outcomes. We return to the
relation of biotechnology to American society in the last section of this
chapter.
v. The question of the knowledge and goodness of goals is often
the neglected topic when people use the language of “mastery,” or “mastery and
control of nature,” to describe what we do when we use knowledge of how nature
works to alter its character and workings. Mastery of the means of intervention
without knowing the goodness of the goals of intervening is not, in fact,
mastery at all. In the absence of such knowledge of ends, the goals of the “master”
will be set rather by whatever it is that happens to guide or move his
will—some impulse or whim or feeling or desire—in short, by some residuum of
nature still working within the so-called master or controller. To paraphrase
C. S. Lewis, what looks like man’s mastery of nature turns out, in the absence
of guiding knowledge, to be nature’s mastery of man. (See his The Abolition
of Man, New York: Macmillan, 1965, paperback edition, pp. 72-80.) There
can, in truth, be no such thing as the full escape from the grip of our
own nature. To pretend otherwise is indeed a form of hubristic and dangerous
self-delusion. For reasons given in the text, therapeutic medicine, though it
may use the same technologies, should not be regarded as “mastery of nature,”
but as service to nature, as we come to know, through medical science, how it
might best be served.
vi. By his very nature, man is the animal constantly looking for
ways to better his life through artful means and devices; man is the animal
with what Rousseau called “perfectibility.”
vii. We have also noted that other people, suffering from certain
neuro-psychiatric disorders, become capable of learning self-control only with
the aid of medication addressed to their disorders.
viii. This is not merely to suggest that there is a disturbance of
human agency or freedom, or a disruption of activities that will confound the
assignment of personal responsibility or undermine the proper bestowal of
praise and blame. To repeat: most of life’s activities are non-competitive;
most of the best of them—loving and working and savoring and learning—are
self-fulfilling beyond the need for praise and blame or any other external
reward. In these activities, there is at best no goal beyond the activity
itself. It is the possibility of natural, unimpeded, for-itself human activity,
that we are eager to preserve against dilution and distortion.
ix. The gift of added years of expected future life is surely a
great blessing for the young. But is the correlative perception of a seemingly
limitless future an equal blessing? How preciously do people regard each day of
life when its limits are out of sight?
x. “Medicalization,” a term coined by sociologists, means in the
first instance a way of thinking and conceiving human phenomena in medical
terms, which then guides ways of acting and organizing social institutions.
More fully, it is the tendency to conceive an activity, phenomenon,
condition, behavior, etc., as a disease or disorder or as an affliction that
should be regarded as a disease or disorder: (1) people suffer it (the
essence of patient-hood) or it befalls them; they are victims of it,
hence not responsible for it; (2) the causes are physical or somatic,
not “mental” or “spiritual” or “psychic”; (3) it requires (needs) and demands
(has a claim to) treatment, aimed at cure or at least relief and
abatement of symptoms; (4) at the hands of persons trained in the healing arts
and licensed as healers; and (5) this conception of the condition will
be supported by the society, which will also support efforts at treatment out
of its interest in the health (as opposed to the morals or the
education) of its people. The term is used—both in the literature and by us
here—as neutral description, without any implied judgment. We have discussed
medicalization of mental life briefly in Chapter Five.
xi. Or without birthmarks, the superficial sign of being marked
from birth as finite and frail. See Nathaniel Hawthorne, “The Birth-mark.”
Endnotes
1. This discussion depends heavily on a paper by Michael J.
Sandel, “What’s Wrong with Enhancement,” prepared for the President’s Council
on Bioethics, Washington, D.C., December 12, 2002. Copy available at the
Council’s website, www.bioethics.gov.
2. The discussion that follows depends heavily on a paper by Leon
R. Kass, “Beyond Therapy: Biotechnology and the Pursuit of Human Improvement,”
prepared for the President’s Council on Bioethics, Washington, D.C., January
16, 2003. Copy available at the Council’s website at www.bioethics.gov.
3. See, for example, Jonas, H., “The Blessings and Burdens of
Mortality,” Hastings Center Report, January/February 1992; Kass, L., “L’Chaim
and Its Limits: Why Not Immortality,” in Life, Liberty, and the Defense of
Dignity: The Challenge for Bioethics, San Francisco: Encounter Books, 2002.
==============================
Bibliography
Abraham, C. “Gene Pioneer Urges Human Perfection.” Toronto
Globe and Mail, 26 October 2002.
American College Health Association. National College
Health Assessment: Reference Group Executive Summary Spring 2002.
Baltimore: American College Health Association, 2002.
American Psychiatric Association. Diagnostic and
Statistical Manual of Mental Disorders. Fourth Edition. Text Revision [“DSM-IV-TR”].
Washington, D.C.: American Psychiatric Association, 2000.
American Society for Reproductive Medicine (Ethics
Committee). “Preconception Gender Selection for Nonmedical Reasons.” Fertility
and Sterility 75: 5, 2001.
American Society for Reproductive Medicine (Ethics
Committee). “Sex Selection and Preimplantation Genetic Diagnosis.” Fertility
and Sterility 72: 4, 1999.
Angold, A., et al. “Stimulant treatment for children: A
community perspective.” Journal of the American Academy of Child and
Adolescent Psychiatry 39: 975-984, 2000.
Aristotle. Nicomachean Ethics.
Aristotle. Rhetoric. trans. L. Cooper, Englewood
Cliffs, N.J.: Prentice-Hall, 1960.
Asakura, A., et al. “Muscle satellite cells are
multipotential stem cells that exhibit myogenic, osteogenic, and adipogenic
differentiation.” Differentiation 68(4-5): 245-253, 2001.
Austad, S. “Adding Years to Life: Current Knowledge and
Future Prospects.” Presentation at the President’s Council on Bioethics,
Washington, D.C. (www.bioethics.gov), 12 December 2002.
Austen, Jane. Mansfield Park, 1814.
Baard, E. “The Guilt-Free Soldier.” Village Voice, 28 January 2003.
Barbaresi, W., et al. “How
common is attention-deficit/hyperactivity disorder? Incidence in a
population-based birth cohort in Rochester, Minnesota.” Archives of
Pediatric and Adolescent Medicine 156: 217-224, 2002.
Barondes, S. Better Than Prozac: The Future of
Psychiatric Drugs. Oxford: Oxford University Press, 2003.
Barton-Davis, E., et al. “Viral mediated expression of
insulin-like growth factor I blocks the aging-related loss of skeletal muscle
function.” Proceedings of the National Academy of Sciences 95(26):
15603-15607, 1998.
Benetos, A., et al. “Telomere length as an indicator of
biological aging: The gender effect and relation with pulse pressure and pulse
wave velocity.” Hypertension 37(2): 381-385, 2001.
Biederman, J., et al. “Pharmacotherapy of Attention-Deficit
Hyperactivity Disorder Reduces Risk for Substance Use Disorder.” Pediatrics
104: e20, 1999.
Blackburn, E. “Telomere states and cell fates.” Nature
408(6808): 53-56, 2000.
Borges, J. “Funes the Memorious” in Ficciones, ed.
John Sturrock, 1942 [English translation, Grove Press, 1962; reprinted by
Knopf/Everyman, 1993].
Bradley, C. “The Behavior of Children Receiving Benzedrine.”
American Journal of Psychiatry 94: 577-585, 1937.
Braude, P., et al. “Preimplantation Genetic Diagnosis.” Nature
Review Genetics 3(12): 941-953, December 2002. (See also erratum, Nature
Review Genetics 4(2): 157, February 2003.)
Braun, S. The Science of Happiness: Unlocking the
Mysteries of Mood. New York: John Wiley & Sons, 2000.
Brown, W. “A method for estimating the number of motor
units in thenar muscles and the changes in motor unit count with aging.” Journal
of Neurology, Neurosurgery, and Psychology 35: 845-852, 1972.
Cahill, L., et al. “Beta-Adrenergic activation and memory
for emotional events.”
Nature 371: 702-704, 1994.
Castellanos F., et al. “Anatomic brain abnormalities in
monozygotic twins discordant for attention-deficit hyperactivity disorder.” American
Journal of Psychiatry 160(9): 1693-1696, 2003.
Castellanos, F., et al. “Neuroscience of
Attention-Deficit/Hyperactivity Disorder: The Search for Endophenotypes.” Nature
Reviews Neuroscience 3: 617-628, 2002.
Cawthon, R., et al. “Association between telomere length in
blood and mortality in people aged 60 years or older.” Lancet 361(9355):
393-395, 2003.
Chan, A., et al. “Foreign DNA transmission by ICSI:
injection of spermatozoa bound with exogenous DNA results in embryonic GFP
expression and live rhesus monkey births.” Molecular Human Reproduction
6(1): 26-33, 2000.
Cohen, E. “Our Psychotropic Memory.” SEED, no. 8, Fall
2003.
Collins, F. “Genetic Enhancements: Current and Future
Prospects.” Presentation at the President’s Council on Bioethics, Washington,
D.C. (www.bioethics.gov), 13 December 2002.
Coyle, J. “Psychotropic drug use in very young children.” Journal
of the American Medical Association, 283(8): 1059–1060, 2000.
Cuttler, L., et al., “Short stature and growth hormone
therapy: a national study of physician recommendation patterns.” Journal of
the American Medical Association 276: 531-537, 1996.
Davis, D. Genetic
Dilemmas: Reproductive Technology, Parental Choices, and Children’s Futures.
New York: Routledge, 2001.
DeGrandre, R. Ritalin Nation: Rapid-Fire Culture and the
Transformation of Human Consciousness. New York: Norton, 1999.
Descartes, R. Discourse on the Method of Conducting One’s
Reason Well and Seeking Truth in the Sciences, 1637.
Descartes, R. The Passions of the Soul, 1649.
Diller, L. “Prescription Stimulant Use in American
Children: Ethical Issues.” Presentation at the President’s Council on
Bioethics, Washington, D.C. (www.bioethics.gov), 12 December 2002.
Diller, L. Running on Ritalin: A Physician Reflects on
Children, Society and Performance on a Pill. New York: Bantam Books, 1998.
Dillin, A., et al. “Rates of behavior and aging specified
by mitochondrial function during development.” Science 298(5602):
2398-2401, 2002.
Dillin, A., et al., “Timing requirements for insulin/IGF-1
signaling in C. elegans.” Science 298(5594): 830-834, 2002.
Dunlop, S., et al. “Pattern Analysis Shows Beneficial
Effect of Fluoxetine Treatment in Mild Depression.” Psychopharmacology
Bulletin 26: 173-180, 1990.
Eberstadt, N. “Choosing the Sex of Children: Demographics.”
Presentation at the President’s Council on Bioethics, Washington, D.C.
(www.bioethics.gov), 17 October 2002.
Eberstadt, M. “Why Ritalin Rules.” Policy Review 94,
April/May 1999.
Elliott, C. Better Than Well: American Medicine
Meets the American Dream. New York: Norton, 2003.
Enge, M. “Ad Seeks Donor Eggs for $100,000, Possible New
High.” Chicago Tribune, 10 February 2000.
Eriksson, M., et al. “Recurrent de novo point mutations in lamin A cause
Hutchinson-Gilford progeria syndrome.” Nature
423: 293-298, 2003.
Fletcher, J. “Ethics and Amniocentesis for Fetal Sex
Identification.” Hastings Center Report, 10(1): 16, 1980.
Fried, S. “Addicted to Antidepressants? The Controversy
Over a Pill Millions of Us Are Taking.” Glamour, April 2003.
Fukuyama, F. Our Posthuman Future: Consequences of the
Biotechnology Revolution. New York: Farrar, Straus and Giroux, 2002.
Gates, D. “The Case of Dr. Strangedrug.” Newsweek,
19 June 1993.
German National Ethics Council. Genetic diagnosis before
and during pregnancy: opinion. Berlin: Nationaler Ethikrat, 2003.
Glader, P. “From the Maker of Effexor: Campus Forums on
Depression.” Wall Street Journal, 10 October 2002, p. B1.
Gladwell, M. “The Sporting Scene: Drugstore Athlete.” New
Yorker, 10 September 2001.
Glass, B. “Science: Endless Horizons or Golden Age?” Science,
171: 23-29, 1971.
Goodman, E. “Matter Over Mind?” Washington Post, 16
November 2002.
Hancock, L. “Mother’s Little Helper.” Newsweek, 18
March 1996.
Hardin, G. “The Tragedy of the Commons.” Science
162: 1243-1248, 1968.
Hawthorne, N. “The Birth-mark,” in Nathaniel Hawthorne,
Tales and Sketches, ed. R. Pearce. New York: Library of America, 1982.
(Originally published in Twice-Told Tales, 1843.)
Healy, D. The Antidepressant Era. Cambridge, MA:
Harvard, 1997.
Homer, The Odyssey.
Hübner, K., et al. “Derivation of oocytes from mouse
embryonic stem cells.” Science 300(5620): 1251-1256, 2003.
Huxley, A. Brave New World, Norwalk, CT: Easton
Press, 1978. (First published 1932.)
Hyman, S. “Pediatric Psychopharmacology.” Presentation at
the President’s Council on Bioethics, Washington, D.C. (www.bioethics.gov), 6
March 2003.
Jonas, H. “The Burden and Blessing of Mortality.” Hastings
Center Report 22(1): 24-40, January/February 1992.
Juengst, E. “What does enhancement mean?” in E.
Parens, ed., Enhancing Human Traits: Ethical and Social Implications.
Washington, D.C.: Georgetown University Press, 1998, pp. 29-47.
Kass, L. “Beyond Therapy: Biotechnology and the Pursuit of
Human Improvement.” Paper prepared for the President’s Council on Bioethics,
Washington, D.C. (www.bioethics.gov), 16 January 2003.
Kass, L. “L’Chaim and Its Limits: Why Not
Immortality” in Life, Liberty, and the Defense of Dignity: The Challenge for
Bioethics. San Francisco, CA: Encounter Books, 2002.
Kessler, R., et al. “Posttraumatic Stress Disorder in the
National Comorbidity Survey.” Archives of General Psychiatry 52(12):
1048-1060, 1995.
Klam, M. “Experiencing Ecstasy.” New York Times Magazine,
21 January 2001.
Klerman, G., et al. “Increasing rates of depression.” Journal
of the American Medical Association 261(15): 2229-2235, 1989.
Knutson, B., et al. “Selective Alteration of Personality
and Social Behavior by Serotonergic Intervention.” American Journal of
Psychiatry 155: 373-379, 1998.
Kramer, P. “Happiness and Sadness: Depression and the
Pharmacological Elevation of Mood.” Presentation at the President’s Council on
Bioethics, Washington, D.C. (www.bioethics.gov), 12 September 2002.
Kramer, P. Listening to Prozac. Second edition. New
York: Penguin, 1997.
Kramer, P. “The Valorization of Sadness: Alienation and the
Melancholic Temperament.” Hastings Center Report 30(2): 13-18, 2000.
Kulka, R., et al. Trauma and the Vietnam War Generation:
Report of Findings from the National Vietnam Veterans Readjustment Study. New
York: Brunner/Mazel, 1990.
Lane, M., et al. “The Serious Search for an Anti-Aging
Pill.” Scientific American 287(2): 36-41, 2002.
Langer, G. “Use of Anti-Depressants Is a Long-Term
Practice.” Abcnews.go.com.<10 April 2003.
Langreth, R. “Viagra for the Brain.” Forbes, 4
February 2002.
Lewis, C.S. The Abolition of Man. New York:
Macmillan, 1965.
LeDoux, J. “Emotion, Memory, and the Brain.” Scientific American
270, 32-39, 1994.
Liotti, M., et al. “Differential Limbic-Cortical Correlates
of Sadness and Anxiety in Healthy Subjects: Implications for Affective
Disorders.” Biological Psychiatry 48: 30-42, 2000.
Locke, J. Essay Concerning Human Understanding. 1690.
Luria, A. The Mind of a Mnemonist: A little book about a
vast memory, trans. L. Solotaroff. New York: Basic Books, 1968.
Mandavilli, A. “Fertility’s new frontier takes shape in a
test tube.” Nature Medicine 9(8): 1095, 2003.
Marshall, E. “Gene Therapy a Suspect in Leukemia-like
Disease.” Science 298: 34, 2002.
Marshall, E. “Second Child in French Trial is Found to Have
Leukemia.” Science 299: 320, 2003.
McGaugh, J. “Emotional Activation, Neuromodulatory Systems
and Memory” in D. Schacter, et al., eds., Memory Distortion: How Minds, Brains, and Societies
Reconstruct the Past. Cambridge, MA: Harvard University Press,
1995, pp. 255-273.
McGaugh, J. “Enhancing Cognitive Performance.” Southern
California Law Review 65(1): 383-395, 1991.
McGaugh, J. “Memory consolidation and the amygdala: a
system perspective.” Trends in Neuroscience 25(9): 456-461, 2002.
McGaugh, J. “Remembering and
Forgetting: Physiological and Pharmacological Aspects.” Presentation at the
President’s Council on Bioethics, Washington, D.C. (www.bioethics.gov), 17
October 2002.
McGaugh, J. “Significance and Remembrance: The Role of
Neuromodulatory Systems.” Psychological Science 1: 15-25, 1990.
McHugh, P., et al. The Perspectives of Psychiatry.
Baltimore: Johns Hopkins, 1998.
Meilaender, G. “Why Remember?” First Things
No. 135: 20-24, August/September 2003.
Montaigne, M. “That to Philosophize Is to Learn to Die” in
The Complete Essays of Michel Montaigne, trans. D. Frame. Stanford, CA:
Stanford University Press, 1965.
Murphy, C., et al. “Genes that act downstream of DAF-16 to
influence the lifespan of Caenorhabditis elegans.” Nature 424: 277-283,
2003.
Musaro, A., et al. “Localized Igf-1 transgene expression
sustains enlargement and regeneration in senescent skeletal muscle.” Nature
Genetics 27: 195-200, 2001.
National Human Genome Research Institute. “News Release:
Researchers Identify Gene for Premature Aging.” Washington, D.C.: National
Institutes of Health (www.genome.gov), 16 April 2003.
National Institute of Mental Health. Medication. Washington,
D.C.: NIH Publication No. 02-3929, 2002.
National Institute of Mental Health. The Numbers Count:
Mental Disorders in America. Washington, D.C.: NIH Publication No. 01-4584,
2003.
National Research Council/National Academy of Sciences,
Committee on Life Sciences and Social Policy. Assessing Biomedical
Technologies: An Inquiry into the Nature of the Process. Washington, D.C.:
National Academy of Sciences, 1975.
National Science Foundation. Converging Technologies for
Improving Human Performance: Nanotechnology, Biotechnology, Information
Technology and Cognitive Science. Arlington, VA: National Science
Foundation, 2003.
Nestler, E., et al. “Neurobiology of Depression.” Neuron
34: 13-25, 2002.
Olshansky, S., et al. “No Truth to the Fountain of Youth.” Scientific
American, June 2002, pp. 92-95.
Owino, V., et al. “Age-related loss of skeletal muscle
function and the ability to express the autocrine form of insulin-like growth
factor-1 (MGF) in response to mechanical overload.” FEBS Letters 505:
259-263, 2001.
Parens, E., ed. Enhancing Human Traits: Ethical and
Social Implications. Washington, D.C.: Georgetown University Press, 1998.
Pinker, S. The Blank Slate: The Modern Denial of Human
Nature. New York: Viking, 2002.
Pinker, S. “Human Nature and Its Future.” Presentation at
the President’s Council on Bioethics, Washington, D.C. (www.bioethics.gov), 6
March 2003.
Pitman, R., et al. “Pilot Study of Secondary Prevention of
Posttraumatic Stress Disorder with Propranolol.” Biological Psychiatry 51: 189-192, 2002.
Plato. “Symposium,” trans. S. Benardete, in The
Dialogues of Plato. New York: Bantam Books, 1986.
Powledge, T., and J. Fletcher. “A Report from the Genetics
Research Group of Hastings Center Institute of Society, Ethics, and Life
Sciences.” New England Journal of Medicine 300(4): 168-172, 1979.
President’s Commission for the Study of Ethical Problems in
Medicine and Biomedical and Behavioral Research. Screening and Counseling
for Genetic Conditions: A Report on the Ethical, Social, and Legal Implications
of Genetic Screening, Counseling, and Education Programs. Washington, D.C.:
Government Printing Office, 1983.
President’s Council on Bioethics. Human Cloning and
Human Dignity: An Ethical Inquiry. Washington, D.C.: Government Printing
Office, 2002. Human Cloning and Human Dignity: The Report of the President’s
Council on Bioethics. New York: PublicAffairs, 2002.
Qu-Peterson, Z., et al. “Identification of a novel
population of muscle stem cells in mice: potential for muscle regeneration.” Journal
of Cell Biology 157(5): 851-864, 2002.
Ramsey, J., et al. “Dietary restriction and aging in rhesus
monkeys: the University of Wisconsin study.” Experimental Gerontology
35(9-10):1131-1149, 2000.
Rapoport, J., et al. “Dextroamphetamine: its cognitive and
behavioral effects in normal and hyperactive boys and normal men.” Archives
of General Psychiatry 37: 933-943, 1980.
Riddle, M., et al. “Pediatric Psychopharmacology.” Journal
of Child Psychology and Psychiatry 42(1): 73-90, 2001.
Rose, S. “‘Smart drugs’: do they work, are they ethical,
will they be legal?” Nature Reviews Neuroscience 3: 975-979, 2002.
Rosenberg, I. “Summary Comments.” American Journal of
Clinical Nutrition 50: 1231-1233, 1989.
Rosenberg, L. “Brainsick: A Physician’s Journey to the
Brink.” Cerebrum 4: 43-60, 2002.
Roubenoff, R., et al. “Sarcopenia: Current concepts.” The
Journals of Gerontology, Biological and Medical Sciences, Series A, 55A,
M716-M724, 2000.
Rousseau, J.-J. “Discourse on the Origin and Foundations of
Inequality (Second Discourse),” trans. R. and J. Masters, in The First and
Second Discourses, ed. R. Masters. New York: St. Martin’s Press, 1964.
Rudman, D., et al. “Effects of human growth hormone in men
over sixty years old.” New England Journal of Medicine 323: 1-5, 1990.
St. Augustine. The Confessions of St. Augustine,
trans. J. Pilkington. Norwalk, CT: Easton Press, 1979.
Sandel, M. “What’s Wrong with Enhancement.” Paper prepared
for the President’s Council on Bioethics, Washington, D.C. (www.bioethics.gov),
12 December 2002.
Santarelli, L., et al. “Requirement of Hippocampal
Neurogenesis for the Behavioral Effects of Antidepressants.” Science
301: 805-809, 2003.
Sapolsky, R. “Will We Still Be Sad Fifty Years from Now?”
in J. Brockman, ed. The Next Fifty Years: Science in the First Half of the
Twenty-First Century. New York: Vintage, 2002.
Schacter, D. “Remembering and Forgetting: Physiological and
Pharmacological Aspects.” Presentation at the President’s Council on Bioethics,
Washington, D.C. (www.bioethics.gov), 17 October 2002.
Schacter, D. The Seven Sins of Memory: How the Mind Forgets and Remembers. New York: Houghton Mifflin, 2001.
Schatten, G., “Assisted Reproductive Technologies in the
Genomics Era.” Presentation at the President’s Council on Bioethics,
Washington, D.C. (www.bioethics.gov), 13 December 2002.
Science Magazine. “Random Samples.” Science
290(5500): 2249, 22 December 2000.
Shakespeare, W. King Henry the Fourth, Part 2.
Shakespeare, W. A Midsummer Night’s Dream.
Sheline, Y., et al. “Hippocampal atrophy in recurrent major
depression.” Proceedings of the National Academy of Sciences 93:
3908-3913, 1996.
Silver, L. Remaking Eden. New York: Avon
Books, Inc., 1998.
Simpson, J., et al. “Sex Selection” in C. De Jonge and
C. Barratt, eds., Assisted Reproductive Technologies: Current
Accomplishments and New Horizons. Cambridge, U.K.: Cambridge University
Press, 2002, pp. 384-396.
Sinsheimer, R., “The Prospect of Designed Genetic Change.” Engineering
and Science Magazine, California Institute of Technology, April 1969.
Slater, L. “Prozac Mother and Child.” New York Times
Magazine, 17 October 1999, pp. 15-17.
Smalley, S., et al. “Genetic linkage of attention-deficit
hyperactivity disorder on chromosome 16p13, in a region implicated in autism.” American
Journal of Human Genetics 71: 959-963, 2002.
Stock, G. Redesigning Humans: Our Inevitable Genetic
Future. New York: Houghton Mifflin, 2002.
Sweeney, H.L. “Genetic Enhancement of Muscle.” Presentation
at the President’s Council on Bioethics, Washington, D.C. (www.bioethics.gov),
13 September 2002.
Swift, J. Gulliver’s Travels,
1726.
Tsien, J., et al. “Genetic
enhancement of learning and memory in mice.” Nature 401: 63-69, 2
September 1999.
Tzankoff, S., et al. “Effect of Muscle Mass on Age-Related
BMR Changes.” Journal of Applied Physiology 43: 1001-1006, 1977.
United States Drug Enforcement Administration. Methylphenidate/amphetamine
yearly production quotas. Washington, D.C.: Department of Justice, 2000.
Vitiello, B. “Psychopharmacology for young children:
Clinical needs and research opportunities.” Pediatrics 108(4): 983-989,
2001.
Vitiello, B. “Stimulant Treatment
for Children: A Community Perspective: Commentary.” Journal of the American
Academy of Child and Adolescent Psychiatry 39: 992-994, 2000.
Vonnegut, K. “Harrison Bergeron” in Welcome to the
Monkey House. New York: Delacorte, 1968.
Wade, N. “Of Smart Mice and an Even Smarter Man.” New
York Times, 7 September 1999.
Wadman, M. “So You Want a Girl?” Fortune, 9 February
2001.
Weber, M. “Effects of growth hormone on skeletal muscle.” Hormone
Research 58(3): 43-48, 2002.
Weindruch, R., et al. The Retardation of Aging and
Disease by Dietary Restriction. Springfield, Ill.: Charles Thomas
Publishers, 1998.
Wheeler, T. “Miracle Molecule, 50 Years On.” Baltimore
Sun, 4 February 2003, p. 8A.
Wilson, J.Q. The Marriage Problem: How Our Culture Has
Weakened Families. New York: HarperCollins, 2002.
Wolterstorff, N. Lament for a Son. Grand Rapids, MI:
Eerdman’s, 1987.
Yesavage, J., et al. “Donepezil and flight simulator
performance: effects on retention of complex skills.” Neurology 59:
123-125, 9 July 2002.
Zammit, P., et al. “The skeletal muscle satellite cell:
stem cell or son of stem cell?” Differentiation 68(4-5): 193-204, 2001.
Zito, J., et al. “Psychotropic Practice Patterns for Youth:
A 10-Year Perspective.” Archives of Pediatric and Adolescent Medicine
157: 17-25, 2003.
Zito, J., et al. “Trends in the prescribing of psychotropic
medications to preschoolers.” Journal of the American Medical Association
283: 1025-1030, 2000.
==============================